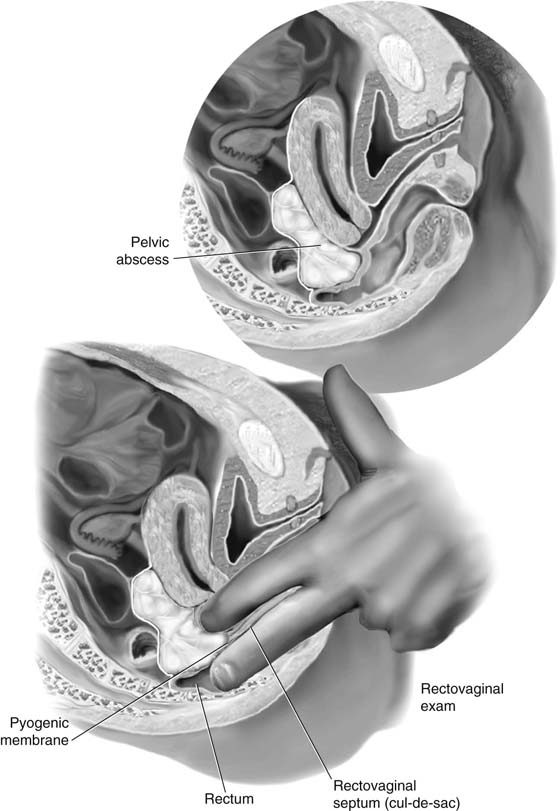
CHAPTER 23 Infections emanating from the tube may result in a variety of abscesses that may require surgical intervention. With the exception of a pelvic abscess, which is typically managed by incision and drainage, tubal abscesses are excised if intensive antibiotic treatment fails to elicit a response. Operative management of these infections utilizes a combination of techniques, including adhesiolysis, salpingectomy, salpingo-oophorectomy, and even hysterectomy. The criteria for drainage of a pelvic abscess are (1) walling-off of the pus (i.e., creation of a pyogenic membrane), and (2) fluctuance (i.e., “pointing” of the abscess just before an anticipated spontaneous rupture). Typically in this location, the pointing process is manifested as the leading edge of the pyogenic membrane dissecting a space within the rectovaginal septum (i.e., between the rectum and vagina). This, of course, is best demonstrated by performance of a rectovaginal examination and palpation of the bulge in the septum. Drainage is performed transvaginally. The cervix is grasped with a single-toothed tenaculum. The vagina has been carefully and gently prepared with povidone-iodine (Betadine) or another suitable surgical preparatory solution. A weighted or Sims retractor is placed along the posterior vaginal wall. Just before incising into the lower cul-de-sac (septum), the surgeon double-gloves and performs a rectovaginal examination to establish the exact position of the rectum relative to the contemplated incision site (Fig. 23–1). Next, an incision is cut into the cul-de-sac. This may be facilitated by careful insertion of an 18-gauge needle attached to a syringe into the abscess and withdrawal of a sample of pus, followed by cutting directly along the track of the needle with a scalpel (Fig. 23–2). As soon as a 1- to 1.5-cm incision is made, the operator’s index finger is inserted into the abscess cavity to (1) provide a guide for enlarging the incision, and (2) break up fibrous septa to enhance drainage (Fig. 23–3). After appropriate culture samples have been obtained and a large rubber drain or two have been inserted into the abscess cavity, and its edges are sutured to the incision edges with 2-0 chromic catgut, a large safety pin is attached to the exposed end of the drain(s) (Figs. 23–4 and 23–5). FIGURE 23–1
Surgery for Pyosalpinx, Tubo-ovarian Abscess, and Pelvic Abscess
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


