Superior Mesenteric Artery Syndrome
Vincent F. Biank
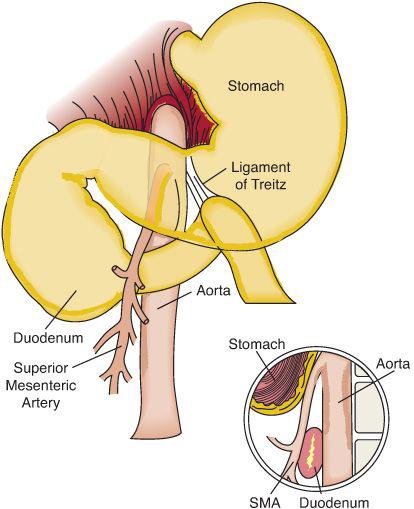
Superior mesenteric artery syndrome (SMAS) is an unusual form of gastrointestinal obstruction resulting from compression of the duodenum between the abdominal aorta posteriorly and the superior mesenteric artery anteriorly (Fig. 406-1).1
 EPIDEMIOLOGY
EPIDEMIOLOGY
The reported incidence of SMAS ranges from 0.01% to 0.3%.4,5,6 SMAS is found more commonly in females than males and typically affects individuals of slender build after acute weight loss, or following orthopedic casting, especially following scoliosis surgery or following the application of a hip-spica cast.7 Acute or chronic neurologic injury is associated with superior mesenteric artery syndrome.8
 PATHOPHYSIOLOGY
PATHOPHYSIOLOGY 
In the majority of the population, the angle between the superior mesenteric artery and the aorta is between 45 and 60 degrees. This angle is in part due to the presence of an anterior mesenteric fat pad, the size of which correlates with body mass index.9 In SMAS, the angle between the aorta and the SMA is reduced to as little as 6 degrees, allowing the SMA to compress the duodenum against the aorta, resulting in mechanical obstruction. 
 CLINICAL FEATURES AND DIFFERENTIAL DIAGNOSIS
CLINICAL FEATURES AND DIFFERENTIAL DIAGNOSIS
Symptoms of SMAS may be acute or chronic. The acute presentation is characterized by symptoms similar to small bowel obstruction, with vomiting, nausea, anorexia, abdominal distention, and abdominal pain.4,8,11 in some individuals the onset is insidious, with symptoms including postprandial epigastric pain, early satiety, and weight loss. In those individuals with abdominal pain, nearly half describe pain as epigastric in location.8
Physical findings are commonly nonspecific but can include abdominal distension, epigastric tenderness, and/or high-pitched bowel sounds.
 DIAGNOSTIC EVALUATION
DIAGNOSTIC EVALUATION
The diagnosis of superior mesenteric artery syndrome (SMAS) is commonly made by upper gastrointestinal radiography that demonstrates a dilated stomach and duodenum with an abrupt cut-off or narrowing of the duodenum at the level of the third lumbar vertebra just proximal to the ligament of Treitz (eFig. 406.1  ). In addition. The diagnosis can also be made by computerized tomography (eFig. 406.2
). In addition. The diagnosis can also be made by computerized tomography (eFig. 406.2  ) or at laparotomy.12,13
) or at laparotomy.12,13
 TREATMENT
TREATMENT
Treatment of superior mesenteric artery syndrome (SMAS) is usually conservative with acute management focused on bowel decompression, maintenance of the fluid and electrolyte balance and nutritional support or rehabilitation. Removal of the body cast as soon as practical is required when SMAS is associated with orthopedic casting.15 Once the patient is stabilized, small, frequent high-caloric oral feeds may be effective. Changes in feeding position (knees to chest or right lateral decubitus positioning) may also be useful in bypassing the obstruction. If symptoms persist, a nasojejunal tube placed past the obstruction allows nutritional rehabilitation for continuous enteral feeding15,16 or parenteral nutrition may be required. In the rare instance where medical treatment fails, surgical intervention may be necessary, particularly when profound chronic dilatation and stasis of the proximal small bowel occurs.15,16
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


