We learn through our senses. What we see, what we hear, what we touch, and what we experience through the perception of movement from our joints and muscles are our foundations for learning. Sensory integration theory is a way of looking at how the brain and the body work together to process sensory stimulation.
Jean Ayres 1994
Sensory processing disorder (SPD) is a Neurodevelopmental Disorder (ND) resulting from the brain’s inability to integrate everyday sensory information received from the five senses: auditory, tactile, taste, olfactory, and visual. The previous are considered to be our “far” senses. In addition to the well known far senses, we have two “hidden” senses through which we receive a vast amount of sensory input: the vestibular and proprioceptive systems. These two senses, along with the interoceptive sense, are our “near senses.” SPD is a term that refers to the way the nervous system receives sensory messages and turns them into responses. With a proper functioning sensory processing system, one has the ability to take in, process, organize, and integrate sensory information so that they feel comfortable and secure. This will then allow one to respond appropriately to given situations and commands/demands both socially and academically. Dysfunction within the sensory integration system can lead to problems with academic learning, motor skills, behavior, and social or emotional development.
The neurological disorganization resulting in SPD can occur in three different ways: (a) the brain does not receive messages because of a disconnection in the nerve cells; (b) sensory messages are received inconsistently; and (c) sensory messages are received consistently but do not connect properly with other sensory messages.
Children with SPD are often misunderstood and may be labeled as aggressive, clumsy, inattentive, or “difficult.” Children dealing with sensory processing issues often say that they are “different” from their friends; they know that they struggle with various academic and social activities that their peers do not. These children often become frustrated with school work because it takes them longer to “get it” or to finish an assignment. They may have poor coordination; therefore, sports and physical education can be difficult and embarrassing for them. Knowing that various physical or academic activities are difficult for them may lead to a child with anxiety and/or depression. Others, primarily boys, may act out their frustration with aggressive and impulsive behavior. Some children may have frequent “meltdowns” when they hit sensory overload.
At the time of this writing, it is estimated that as many as one out of 20 children may suffer from SPD (1) with an estimated 5 to 10% of “normal” children requiring some intervention. SPD can be a stand alone condition or can coexist with attention deficit disorder (ADD), attention deficit hyperactivity disorder (ADHD), or other diagnoses under the umbrella of autism spectrum disorder (ASD) or various neurodevelopmental disorders (NDs). Therefore, treating the sensory processing component in children with the aforementioned disorders may have a positive overall affect on children who also are diagnosed with any of these disorders. Children can be misdiagnosed as having ADD, ADHD, or other disorders along the autism spectrum when their true condition is actually that of SPD. Because children with SPD have characteristics in common with or similar to these disorders, it can be difficult to obtain an accurate diagnosis. Another reason for misdiagnosis is the fact that parents often want a name or “label” for what is wrong with their child. So, if a child has characteristics similar to a certain disorder, for example ADHD, then to satisfy the parent, an evaluating doctor may place a label of ADHD on a child. The fact that SPD is not yet widely known or understood by much of the medical and educational communities and, at the time of this writing, is not yet an official diagnosis on the Diagnostic and Statistical Manual of Mental Disorders IV schedule, many physicians may not use the diagnosis of SPD. With the vast amount of research and clinical documentation to date, a valiant effort is being made to have SPD placed on the Diagnostic and Statistical Manual of Mental Disorders IV schedule by 2012. SPD is currently recognized by and included in the Diagnostic Manual for Infancy and Early Childhood of the Interdisciplinary Council on Developmental and Learning Disorders and the Diagnostic Classification of Mental Health and Developmental Disorders of Infancy and Early Childhood, Revised (DC:0-3R). Common disorders that coexist with SPD are shown in Table 24-1.
TABLE 24.1
Sensory Processing Disorder and Coexisting Conditions
Autism spectrum disorders
ADD/ADHD
Down syndrome
Cerebral palsy
Traumatic brain injury
Fragile X syndrome
Mental retardation
Premature birth
Substance abuse babies
Fetal alcohol syndrome
Bipolar disorder
Oppositional defiant disorder
“Emotionally disturbed”
Conduct disorder
OCD
Learning disabilities
Reactive attachment disorder
CLASSIFICATION OF SPD SUBTYPES
SPD is a global term that has three primary diagnostic subtypes. Type I is sensory modulation disorder (SMD); type II is sensory-based motor disorder (SBMD); and type III is sensory discrimination disorder (SDD).
Type I: Sensory Modulation Disorder
Jean Ayers defined modulation as “the process of increasing or reducing activity to keep the activity in harmony with all functions of the nervous system.” In normal sensory modulation, one should subconsciously be able to create a balance of inhibitory and excitatory input into the central nervous system (CNS) from incoming sensory stimulation. Children with SMD either have too little or too much “toning down” of sensory input into the CNS. Sensory modulation responses may vary depending on the situation and type of sensory input. There are three classic subgroups of SMD: (a) sensory overresponsivity (SOR), (b) sensory underresponsivity (SUR), and (c) sensory seeking (SS).
Sensory Overresponsivity Sensory overresponsivity, often referred to as sensory defensiveness, is a tendency to respond to sensory input faster, more intensely, and for a longer duration. These children have too little “toning down” of sensory information to the CNS; therefore, sensory stimuli into the brain is exaggerated and overwhelming and these children will be hypersensitive to sensory input. These children tend to have difficulty with transition of one activity to another or one environment to another because they are fearful of what additional or different sensory challenges those changes may bring. An example of such a child is one that refuses to transition from circle time to recess or self-play to group play. Examples of SOR in relation to the various individual sensory systems are listed in Table 24-2. A child may have dysfunction within just one of the sensory systems; however, it is common that more than just one sensory system is involved. A child also does not have to display all characteristics within a certain category for there to be dysfunction within that particular sensory system. Making it even more difficult to ascertain a child’s sensory issues is the fact that a child may not always be consistent in the type of behavior or characteristics that he or she displays. Much of the child’s behavior will depend on the level of sensory input/overload and the environment. This can make it more difficult to determine a particular pattern of characteristics. For example, a child may have auditory hypersensitivity but does fairly well in his or her classroom environment because he or she is familiar with what sounds are generally present. The auditory threshold in that particular classroom may be on the high end for that child, but he or she is able to perform academically and socially. It is almost as though the child is able to accommodate to that particular environment. However, if a hyperverbal child is added to the classroom, thus, adding more auditory input to the environment, this child may no longer be able to accommodate and his or her behavior or learning becomes an issue. A child may also have mixed sensitivity and at times display hypersensitivity characteristics while at other times display hyposensitivity characteristics. It has been suggested that a child might display hypersensitive characteristics to sensory stimulation until a point of overload is reached, leading to a shutdown in processing of sensory input. The shutdown then leads to hyporesponsive behavior (2). It is important to understand that everyone has sensory issues from time to time because one cannot stay well regulated all the time; however, if a child’s everyday activities and/or social interactions are affected, then it becomes a disorder that needs to be addressed.
TABLE 24.2
Signs of Sensory Overresponsivity
Auditory
Frequently covers ears, especially in loud environments
Runs away, cries, and/or covers ears with loud or unexpected sounds
Is bothered by or distracted by background environmental sounds, e.g., lawn mower, loud cars, horns, construction, music
Requests quiet environment, i.e., stop making noise, talking, or singing
May be easily distracted by sounds not noticed or bothered about by others such as clocks ticking, air conditioners, refrigerators, fans, etc.
May refuse to go to events/activities where there is a lot of noise such as parties, movie theaters, parades, musical concerts, etc.
Olfactory
Tells other people (or talks about) how bad or funny they smell
Refuses to eat certain foods because of their smell
Is bothered by, gets sick, or has behavioral issues after the use of household cleaning products
Notices and/or reacts negatively to smells which do not usually bother, or get noticed by, other people
Is bothered by or gets irritated by the smell of perfumes, lotions, cologne, candles, etc.
May decide to like/dislike a certain environment by the way it smells Tactile
As an infant, did/does not like to be held or cuddled; may arch back, cry, and pull away
Becomes distressed when diaper or clothes are changed
As a toddler, may have preferred/prefers to be naked and pull diapers and clothes off constantly
Appears fearful of or avoids standing in close proximity to other people or peers such as in groups, crowds, or lines
Is fearful, anxious, or aggressive with light or unexpected touch
Is excessively ticklish
May overreact to minor cuts, scrapes, and or bug bites
Becomes distressed about having hair brushed; may be very picky about using a particular brush
Resists friendly or affectionate touch from anyone besides parents or siblings (and sometimes them too!)
Avoids touching certain textures of material: rough/silky/scratchy, etc.
Becomes distressed or may refuse to walk barefoot on grass or sand
May walk on toes only or only when barefoot and with certain surfaces
Refuses to wear certain clothes such as clothes with rough textures, turtlenecks, jeans, hats, or belts, etc.; distressed by seams in socks and may refuse to wear them
Avoids or dislikes “messy play,” i.e., sand, mud, water, glue, Playdoh, slime, etc.
Is a picky eater, only eating certain tastes and textures; mixed textures tend to be avoided as well as hot or cold foods; resists trying new foods
Becomes distressed when having face washed
Resists brushing teeth and is extremely fearful of the dentist
Taste
Picky eater, often with extreme food preferences, i.e., soft foods, crunchy foods, hot food, cold food, etc.
May only eat “soft” or pureed foods past 24 months of age
Has difficulty with sucking, chewing, and swallowing
Avoids seasoned, spicy, sweet, sour, or salty foods; prefers bland foods
Extreme resistance to trying new/different foods
Easily gags with textured foods
Dislikes or complains about toothpaste and mouthwash
Extreme resistance or fear of going to the dentist or having dental work done
Visual
Avoids eye contact
Is easily distracted by other visual stimuli in the room, i.e., movement, decorations, toys, windows, etc.
Rubs eyes, has watery eyes, or gets headaches after reading, writing, computer use, or watching TV
Is sensitive to bright lights; will squint, cover eyes, cry, and/or get headaches from the light
Will have difficulty in bright colorful rooms or a dimly lit room
Has difficulty keeping eyes focused on task/activity he/she is working on for an appropriate amount of time
Vestibular
Gets motion sickness often or easily, i.e., cars, elevators, head movement
May have disliked being placed on stomach as an infant
As an infant, may never have liked baby swings or jumpers
Dislikes or is fearful of walking on uneven surfaces or going up and down stairs
Avoids/dislikes playground equipment, i.e., swings, ladders, slides, or merry-go-rounds
Does not like activities where feet leave/don’t touch the ground
Prefers sedentary tasks
Does not like spinning or fast movements; avoids rapid or rotating movements
Moves slowly and cautiously, avoids taking risks, and may appear “wimpy”
Does not like head movement, especially in extension, i.e., washing hair
Avoids/dislikes elevators and escalators
Afraid of heights, even the height of a curb or step
Has difficulty with or is fearful of activities that require balance
Loses balance easily
May be fearful of and have difficulty riding a bike, jumping, hopping, skipping, or balancing on one foot (especially if eyes are closed)
Proprioception
Has low muscle tone; limp, “floppy” body
Fatigues easily
May have difficulty turning doorknobs and handles, and opening and closing items
May have never crawled as a baby
Has poor body positional awareness; bumps into things, knocks things over, trips, and/or appears clumsy
Has poor gross motor skills: jumping, catching a ball, jumping jacks, climbing a ladder, etc.
Poor fine motor skills: difficulty using “tools,” such as pencils, silverware, combs, scissors, etc.
Does not establish hand dominance by 4-5 year old; may appear ambidextrous, frequently switching hands for throwing, coloring, cutting, writing, etc.
Has difficulty learning exercise or dance steps
Sensory Underresponsivity Sensory underresponsivity is a tendency to not respond to sensory input, take longer to react to sensory input, and require intense and/or long lasting sensory stimulation before it registers into the CNS.
Sensory underresponsivity children often injure themselves without knowing it because they have such a high pain tolerance. These are children who may present in the chiropractic office and, upon palpation over a severely subluxated atlas that one would expect to be tender or painful, would have little or no reaction. These children tend to be more socially withdrawn and prefer to play alone. They may also be more passive, difficult to engage in conversation, appear to be apathetic with little inner drive, and often tend to be tired. As a baby they may have been described as an “easy baby,” very mild tempered and slow to arouse.
Sensory Seekers Some degree of SS is normal in children as they learn, grow, and develop. However, one must be able to distinguish between what is normal and what is excessive or not adequate. Children who are sensory seekers have an unquenchable craving for sensory input and will seem to seek out sensation almost constantly. This may be in a nonsocially acceptable manner. They are often known as risk takers because they attempt to provide the sensory input they crave. These children can also have very aggressive and invasive personalities and often earn the title of “troublemaker” or “bully.” The type of sensation that they seek out will depend on which sensory systems are deficient. Some general characteristics observed in sensory seekers are follows:
Inability to stay still; must constantly be on the move (vestibular)
Loves to swing or spin or watch spinning things, almost excessively (vestibular)
Likes to push, pull, punch, pinch, kick, or crash into things (proprioceptive)
Takes excessive risks, such as climbing trees or high objects; likes to climb and jump off high places (proprioceptive)
Speaks excessively and often in a loud voice (auditory)
Likes the television or music loud (auditory)
Likes to constantly touch people or items (tactile)
Likes to eat foods that have strong tastes/flavors, such as lemons, peppers, and onions (taste)
Type II: Sensory-Based Motor Disorder
SBMD occurs when there is dysfunction within the vestibular and proprioceptive systems. SBMD has two subtypes: postural disorder and dyspraxia.
Postural Disorder Postural disorder is a problem with posture and postural control as a result of a deficiency in vestibular and proprioceptive processing. These children have low extensor muscle tone, poor core stability, and appear “floppy.” They also have poor equilibrium reactions. As chiropractors, we will see these children in our offices displaying poor posture; they have trouble sitting up straight and tend to slump. The handwriting of these children may be illegible and messy because of the low muscle tone in their hands, arms, and shoulders. Because of their low muscle tone, normal activities take a lot of energy, and these children tend to fatigue easily as their bodies utilize so much extra energy trying to get through a day.
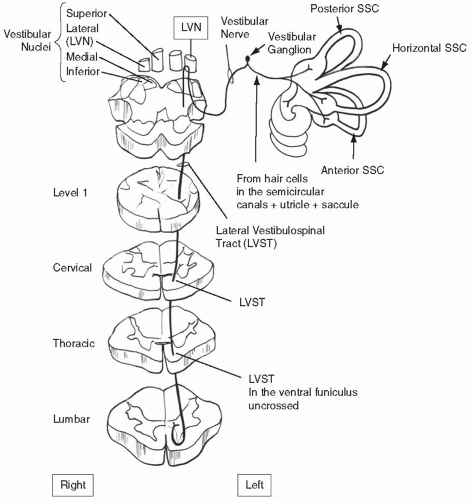
Vestibular and Proprioceptive Processing in Postural Disorder Vestibular and proprioceptive processing are hypothesized to contribute jointly to the perception of active movement; the development of body schema; and the development and use of postural responses, especially those involving extensor muscles (2). There are direct connections found between the vestibular nuclei and the cerebellum, oculomotor nuclei, and the spinal cord. Projections to the spinal cord are sent via the lateral vestibulospinal track (LVST) and medial vestibulospinal tract (MVST). Both of these tracts are responsible for influencing muscle tone as well as maintaining postural adjustments. The LVST has fibers that terminate in the spinal cord at the cervical, lumbar, and sacral regions. The alpha motor neurons of the LVST supply muscle fibers while the gamma motor neurons project to the muscle spindles. Therefore, the vestibular system has a strong influence on postural muscles, postural control, and postural stability. The MVST receives input from the cerebellum and from skin and joint proprioceptors. Fibers from the MVST project to the flexor and extensor motor neurons in the cervical region of the spinal cord. These fibers are responsible for assisting with maintaining a consistent position of the head in space. Therefore, with descending vestibular projections, we see the connection between vestibular and proprioceptive input. Some manifestations in children with posture disorder are as follows:
Poor endurance; fatigues easily
Does not have a consistent dominant side; that is, switches dominant hand
Is not able to contract muscles against resistance
Has difficulty with crossing the midline activities
Has poor balance
Is “weak” or “wimpy”
Has difficulty climbing or pulling him- or herself up; that is, chin ups, push-ups, jungle gyms
Dyspraxia Dyspraxia is a problem in planning, sequencing, and executing novel motor actions as a result of sensory dysfunction. Children with dyspraxia will have difficulty with motor tasks or activities requiring multiple steps. Dyspraxia is usually not detected within the first 3 years of life and children will usually achieve normal motor milestones but at the latter end of the age ranges. Preschool and elementary school are often when dyspraxia starts to become a noticeable problem. This is because tasks must be completed in specific time periods and there are more expectations of neatness and organization. Also, children may now be required to participate in activities that they were previously able to avoid because they were too difficult and/or frustrating. Parents often become frustrated by the child’s inconsistencies in performance and blame the child’s behavior on disobedience, laziness, or carelessness. Children with dyspraxia often become easily frustrated and give up when attempting various activities. They will often suffer from low self-esteem because of their inability to perform various tasks that may be easy for their peers. Subtypes of dyspraxia are gross motor dysfunction, fine motor dysfunction, or oral motor dysfunction. A child may have one subtype of dyspraxia or a combination of the subtypes.
Bilateral Integration and Sequencing Bilateral integration and sequencing (BIS) is the ability to use the two sides of the body in coordinated fashion and sequencing motor actions for gross motor skills. Bilateral assistive skills such as activities where one hand must act as a stabilizer and the other as the primary “doer” are difficult. Reciprocal bilateral body movements such as jumping or skipping or using the hands to drum are often lacking or nonexistent. The child will also tend to have a strong resistance to activities that require crossing the midline. It is a type of sensory integrative based dyspraxia in which there are deficits in vestibular and proprioceptive processing. Children with BIS will display gross motor dyspraxia and tend to be awkward and clumsy. They will often have difficulty with sports and physical education classes can seem like torture to these children. Some signs of BIS follow:
Right/left confusion
Poor lateralization of upper extremity
Avoidance of crossing the midline
Poor ability to do activities such as skipping, jumping jacks, and catching and throwing a ball
Slow to sit up, roll, crawl, or reach other gross motor milestones
Difficulty with activities that require more than one step
Poor organizational skills, often exhibited has messy bedroom and school work is not organized
Clumsy, uncoordinated appearance and difficulty learning new motor tasks
Struggles with bike riding and using playground equipment
Trouble conceiving, organizing, and performing activities that involve a sequence of body movements
Trouble with new experiences as well as familiar ones
Poor hand-eye coordination
Somatodyspraxia Children with somatodyspraxia will have difficulty with simple and difficult motor tasks as well as with fine motor tasks. They will have a deficit in the somatosensory system, which encompasses tactile and proprioceptive sensory information. In addition, they may have vestibular processing issues. Fine motor dyspraxia starts to become noticeable around 1 year of age, when children may have difficulty picking up, letting go, or holding small objects such as Cheerios. As toddlers, they may have trouble staying inside the lines when coloring. Elementary age children may have trouble with self-care activities and their handwriting may be sloppy and difficult to read. Difficulty in self-care activities continues to become more noticeable and often turns into morning battles and “running late.” Children with somatodyspraxia will have the same signs as those with BIS, as well as the following:
Difficulty with self-care: fastening buttons, blowing nose, etc.
Struggles with toys and play activities such as: puzzles, cut and paste
Difficulty with handwriting
Poor fine motor control of fingers for precise manual tasks and/or of toes for gripping sandals or walking barefoot
Oral Motor Dyspraxia Oral Motor dyspraxia is the ability to organize sequenced movements in the area of the mouth, tongue, and lips. Naturally, it is often a problem area for children with speech disorders. Drooling can often be a problem because the child’s jaws may hang open. Chewing and eating, as well as tasks such as blowing bubbles, and whistling, can be problematic. An older child or adult may have difficulty with reading that is associated with oral praxis. They may be unable to sequence sounds and be unable to sound out the word properly. Information from the sense of touch is especially important for good oral praxis. Signs of oral motor dyspraxia include:
Messy eater
Drooling
Poor fine motor control of the mouth muscles for chewing and speaking
Type III: Sensory Discrimination Disorder
SDD refers to the inability to interpret the quality of sensory information or distinguish messages within a particular sensory system. Children with SDD may have difficulty with sensory interpretation because the sensory input is either jumbled or not received at all. They also have a decreased ability to interpret the spatial or temporal qualities of the various sensory systems. SDD is thought to play a role in praxis because of its underlying association with poor body schema (i.e., body positional awareness). Dysfunction of SDD tends to be more of a constant in comparison to SMD, which can fluctuate from day to day or situation to situation. Children with SDD take longer to process the sensory information that they perceive, which can make them seem to be cognitively delayed. This can lead to frustration and low self-esteem for the child. Examples of SDD are as follows:
Inability to tell what is in their hand without looking, for example, distinguishing between a penny and a dime in their pocket
Inability to tell what is touching them and where it is on their body
Difficulty differentiating food textures
Difficulty differentiating or identifying smells
Difficulty differentiating or identifying sounds; for example, neck from nag
Difficulty knowing if they are in motion or not; that is, only knows up from down by knowing where their head is
Difficulty knowing how much force to use; for example, how much force to use when holding a pencil and writing
Inability to discriminate visually between b’s and d’s or q’s and p’s, etc.
Causes of SPD
Like other NDs, a specific cause or causes of SPD are not yet known. Preliminary reports and research suggest that environment, birth trauma, toxicity exposure, and hereditary factors are all likely contributors. Another contributing factor may be that of overactivation of the sympathetic nervous system. It is likely that the cause of SPD and other NDs is a combination of factors. It is known, however, that, at the root of its dysfunction, SPD is the result of an immature or atypical development of the nervous system.
Environment The environment of the developing child is extremely important in nurturing a healthy sensory processing system. An environment where there is little or no sensory stimulation during childhood can lead to a poorly developed or weak sensory processing system; thus, these children will display abnormal sensory patterns. Studies of children living in Romanian orphanages find a strong correlation between future sensory processing issues and environments with low levels of sensory stimulation. One study (3) examined the relation between length of institutionalization and sensory integration in children adopted from Eastern Europe. The study concluded that longer lengths of institutionalization are associated with more atypical sensory discrimination, praxis, and sensory modulation scores among children adopted from Eastern European orphanages. The areas of sensory integration that appear to be most vulnerable to deprived conditions are vestibular, proprioceptive, tactile, visual, auditory, and praxis.
Birth Trauma Another theoretical cause or contribution of SPD is birth trauma from breech presentation, use or forceps or vacuum extraction, or Cesarean section. Correlation to children with sensory symptoms and prolonged labor, induction, prematurity, and fetal distress have also been noted. In one study of children with sensory symptoms, prolonged labor, fetal distress, forceps/vacuum delivery, and jaundice all occurred at a much higher rate than among the general population (4).
Breech deliveries are said to cause damage more frequently to the structures of lower cervical and upper thoracic spine while forceps deliveries may involve an increased risk of injury to the upper cervical structures. One must also consider trauma during a “normal” birth. Axial pressure is the force encountered in a normal birth; the pressure forced onto the cervical spine can be attributed to strong contractions, manual pressure, or hormonal enhancement of the natural contractions. All can lead to subluxation of the atlas into the foramen magnum with disruption of the cerebellum (5). Refer to Chapters 6 and 7 for additional information about birth trauma.
Toxicity Exposure There are two types of toxins of concern in children with SPD and other NDs: (a) exogenous toxins and (b) endogenous toxins.
Exogenous toxins are toxins that come from outside sources such as heavy metals, pesticides, cleaning agents, polychlorinated biphenyls, and other such pollutants. Mercury in particular is said to have an affinity for brain cells. Food additives, such as food colorings, preservatives, monosodium glutamate, and aspartame/phenylalanine are said to be neurotoxins and can accumulate in cells and tissues of the body and brain. Fetal drug (prescription or recreational) and alcohol exposure are also of concern.
Endogenous toxins are toxins within the body, such as metabolic waste, bacterial by-products, and toxic matter within the gut. Micro-organisms, such as viruses, bacteria, fungi, and parasites, can invade and then propagate within the body. If detoxified and kept within healthy limits, these organisms are not of concern. Hormones, ammonia, and yeast are examples of metabolic end products that are part of the natural function of our body; however, if they are not metabolized and expelled properly, they too become toxic to the body.
Heredity One small pilot study (4) explored the possibility of family links between 27 children and their biological parents: 18 boys and nine girls. The correlation was so pronounced that it was not necessary to trace the disorder through generations, as is often the case in hereditary studies. The study showed that all except one boy and one girl had at least one parent with SPD symptoms. The association when the mother had symptoms of SPD was 40% whereas the association when the father had symptoms of SPD was 37%. The results of the pilot study suggests a hereditary link; thus, there is a need for a larger study. A study of twins done by Goldsmith (6) at the University of Wisconsin-Madison studied 1,394 toddler-aged twins for tactile and auditory defensiveness as reported by mothers. Twin correlations for the full range of scores and concordance rates for the extremes suggested a moderate influence for genetic factors, with some suggestion that the tactile domain might be more heritable and that genetic influence might increase with severity. Identical twins were found to be much more likely to have the same sensory symptoms than were nonidentical twins. These findings also suggest that there is a hereditary link with SPD.
Autonomic Nervous System
Children who are overresponsive to sensory stimulation demonstrate behaviors that are consistently fight-or-flight responses. These children will have an exaggerated reaction to sensory stimulation and a delayed or absent calming reaction. They are described as being “sensory defensive” because they have a strong negative reaction to sensory stimuli that most of us do not perceive as being harmful or negative. Thus, they may appear to overreact in various situations depending on the stimuli or they appear constantly distracted or fidgety. The working theory with overresponsive sensory children is that the neurological balance between the parasympathetic and sympathetic nervous system is not functioning effectively; thus, these children tend to operate in sympathetic overdrive. McIntosh et al. (7) demonstrated differences in electrodermal response (EDR) measures between children with and without SPD; EDR was measured by recording sweat responses to various sensory stimuli. Ten trials were conducted for the following sensory stimuli: olfactory, auditory, visual, tactile, and vestibular. Children with SPD showed more and larger EDR than the control group. Participants with sensory disturbances habituated more slowly to repeated stimulation, as measured by the number of responses to stimuli and proportion of stimuli that evoked responses. Children with atypical EDR had more parent-reported abnormal behavioral responses to sensory stimuli. Children with clinically identified SPD respond physiologically differently to sensory stimuli than typically developing children; these differences have ramifications for functional behavior. A similar pilot study (8) was performed in 2001 measuring EDR along with cardiac vagal tone. Vagal stimulation slows the rhythm of the sinus node while simultaneously decreasing the excitability of the intermodal pathways, with the net result being a slowing of the heart rate. The study found that children with SPD had less effective parasympathetic functions than typically developing children and showed significantly lower vagal tone than normal developing children. There are various studies that suggest individuals who have greater vagal influence are quicker to respond to stimuli, respond more strongly, calm down again more quickly, and are more emotionally expressive than individuals whose vagal tone and capacity for vagal suppression is lower. In another such study (9), it was found that poorer modulation for vagal tone was associated with greater social anxiety, whereas lower vagal tone across recording periods was associated with greater defensiveness and lower behavioral activation sensitivity. In another study by Porges et al. (10), data from 24 infants found support for the model that infants with difficulties in decreasing vagal tone during social/attention tasks at 9 months of age had significantly more behavioral problems at 3 years of age. Most of the research in this arena has focused on the overactive sympathetic nervous system and overresponsive sensory children. However, the possibility of an underactive parasympathetic nervous system in hyporesponsive children has also been explored but not to the same extent.
Regarding the autonomic nervous system, the doctor of chiropractic may have the ability to influence the balance between the parasympathetic and sympathetic nervous system by removing interference caused by vertebral subluxation. For example, a subluxation of the upper cervical spine may hinder the function of the parasympathetic nervous system, thus allowing for overactivation of the sympathetic nervous system. In a 2001 study, Budgell and Hirano (11) evaluated heart rate changes in 25 young adults after sham and real chiropractic adjustments to the upper cervical spine. They showed that stimulation of the neck via spinal manipulation is capable of eliciting changes in heart rate; specifically, it resulted in inhibition of the sympathetic nervous system. In a 2002 study, Koch et al. (12) monitored the heart rate of infants before, during, and after the application of a unilateral mechanical impulse (spinal adjustment) to the upper cervical spine. The most frequent neurological finding was a decreased heart rate. As with Budgell and Hirano (11), this is consistent with inhibition of the sympathetic nervous system. For more information on the regulation of the sympathetic and parasympathetic nervous system, refer to Chapter 9.
The Cerebellum
The function of the cerebellum is a vital component when dealing with children with SPD or any other ND. It will be addressed briefly in this chapter and more so in Chapter 25, which examines other NDs. The cerebellum begins development by the sixth month of pregnancy. Its largest growth spurt is in the first 2 years after birth, but continues to grow and change into adolescence. The archicerebellum is located at the base of the cerebellum. It is an evolutionary outgrowth of the vestibular system, from which certain fibers pass directly to the cerebellar cortex. The majority of fibers relay information via the vestibular nuclei and the reticular activating system (RAS) in the brainstem. The paleocerebellum receives action potentials from the skin, joints, and primary endings of the neuromuscular spindles; thus, it has tactile and proprioceptive (somatosensory) connections. Its function is that of progressive movement (e.g., standing, walking, running) and it is concerned with posture, muscle tone, and gait. The neocerebellum is functionally related to the corticopontocerebellar system, which is chiefly involved in voluntary motor control. It plays a major part in the control of hand and mouth movements and is therefore also involved in speech, articulation, and the fine control of manipulative skills such as handwriting. The cerebellar nuclei represent the sole output from cerebellar circuits, bringing signals to brainstem nuclei, thalamic nuclei, motor cortex, premotor cortex, and prefrontal association cortex via the cerebellothalamocortical tract. Each cerebellar nucleus has a complete map of the body, with head located posteriorly, limbs medially, and trunk laterally. The dentate nucleus is the primary output structure of the cerebellum and projects to various areas of the cerebral cortex, such as premotor, prefrontal, posterior parietal, and primary motor cortex mainly via the thalamus. The cortex then sends projections back to the cerebellum via the pons.
The cerebellum is known to play a role in motor learning because cerebellar circuits are modified through experience; essentially, it learns by doing. Cerebellar circuitry controls rate, smoothness, and coordination aspects of movement. As an act is practiced repeatedly so that it can be done with more proficiency and less conscious attention, it will transfer motor tasks from the conscious to the unconscious. Cerebellar input exerts a facilitatory drive upon the contralateral cerebral cortex. Therefore, cerebellar lesions depress the excitability of the contralateral motor cortex. In recent years, the role of nonmotor function of the cerebellum has been researched. Recent anatomical studies show that the output from the cerebellar nuclei also sends projections to nonmotor areas of the prefrontal and posterior parietal cortex in addition to the cortical motor areas. The cerebral cortical area that is the main target of each output area is also a major source of input to the channel. Thus, a closed-loop circuit makes up the interactions of the cerebrocerebellar connections (13). Therefore, the cerebellum is closely linked to sensory as well as motor systems. Impaired functional interaction between the cortical areas and the cerebellum may be involved in a number of symptoms that can be considered disorders of sensorimotor integration. In one study, the researchers state that subtle impairment of motor coordination and sensory integration functions is frequently found in schizophrenia. Clinically, these deficits present as neurological soft signs (NSS). Because of its crucial role in motor function, control of muscle tone and equilibrium, the cerebellum is likely to be involved in the appearance of NSS. Magnetic resonance imaging was performed in 30 patients with firstepisode schizophrenia and 21 healthy controls. NSS were rated on the Heidelberg scale. By manual tracing, the cerebellum was divided into the following subregions bilaterally: anterior lobe, superior posterior lobe, inferior posterior lobe, and corpus medullare, respectively. Volumetric measures were compared between the two groups and related to NSS scores. NSS scores were significantly higher in patients than in controls. Cerebella of patients were significantly smaller with atrophy pronounced in the corpus medullare bilaterally. In the group of patients with schizophrenia, higher NSS scores were found to be related to reduced volumes of the posterior lobes of the cerebellum. In contrast, no significant associations between NSS scores and cerebellar subregions in healthy subjects arose. These findings support the hypothesis of cerebellar involvement in schizophrenia and indicate that alterations in distinct cerebellar regions are related to NSS (14). In a study looking at the corticocerebellar auditory connection, the evidence suggests that interference with cerebellar output by repetitive transcranial magnetic stimulation modifies functional activity associated with cortical auditory processing (15). Pastor et al. (16) studied steady-state visual-evoked responses. Their findings suggested that the amplitude of the steady-state visual-evoked responses corresponds to increased synaptic activity, specifically in Brodmann’s area 17. In addition, they showed that visual stimulation at 40 Hz causes selective activation of the macular region of the visual cortex, and that a region in the dorsal aspect of the crus Ilobule of the left cerebellar hemisphere is activated during repetitive visual stimulation (16). Other tasks associated with the cerebellum include tasks designed to assess attention, executive control, language, working memory, learning, pain, emotion, and addiction. The final “linking” between the cerebellum, the vestibular apparatus, and corpus callosum takes place around ages 7 to 8 years. Number and word reversals in reading and writing are normal until about age 8; however, continued reversal may not be merely dyslexia but may also suggest vestibular and/or cerebellar immaturity.
Auditory System
Listening is a very complex process that involves not just hearing but also processing sounds. Sound itself is multidimensional and is comprised of intensity (loudness, measured in decibels), frequency/pitch (number of sound waves per second), duration (how long the sound waves continue), and localization (from which direction the sound is coming). Children with auditory processing issues, often called central auditory processing disorder, hear normally; however, it is the processing of what they hear that is the problem. They have trouble integrating the multidimensional components of hearing and there is a neurological “mix-up” with the signal of sound as it travels to the brain. The inferior colliculus in the brain stem receives essentially all auditory input and is a major integrating center for the auditory system. It is also connected with the startle reflex (Moro reflex) and the vestibulo-ocular reflex (VOR). The main nucleus of the inferior colliculus is the central nucleus where the cells are sensitive to both timing and intensity differences in the transmission of sound received. The paracentral nucleus of the inferior colliculus receives auditory input as well as input from the spinal cord, dorsal column (tactile and proprioception), and the superior colliculus (SC) (visual processing). The paracentral nucleus is thought to play a role in multisensory integration and auditory attention (Fig. 24-1).
Receptors for the auditory system are located in the cochlea, the core component of which is the organ of Corti. Hair cells are the sensory cells that are located in the organ of Corti. The cochlea is filled with a watery liquid that moves in response to the vibrations coming from the middle ear via the oval window. As the fluid moves, thousands of hair cells are set in motion and convert that motion to electrical signals that are communicated via neurotransmitters to many thousands of nerve cells. These primary auditory neurons transform the signals into action potentials that travel along the auditory nerve to structures in the brainstem for further processing. Hair cells are also the receptors in the vestibular system; the mechanism of transduction from hair cell receptors of the auditory system is similar to that of the vestibular system. This is why auditory processing and vestibular processing are so intimately linked; they are both situated in the inner ear, their sensory receptors work the same way, they have common fluids, they depend on the same nerve, and they share some of the same nerve fibers. Every time one hears a sound, it activates their gravity receptors, and any time one moves, it activates their auditory receptors. Sensory-based auditory processing deficit is frequently found in children with ASD, developmental delays, learning disorders, and ADHD. Children with sensory-based auditory processing deficits will often have speech and language disorders or difficulties. It has been shown that vestibular input can be an important factor in speech development and can be therapeutic among children with developmentally delayed speech (17,18). Children with sensory-based auditory processing deficit may have a history of repeated ear infections, have an unusually high or low voice volume, or have trouble with reading or spelling. Refer to Tables 24-2 and 24-3 for additional characteristics of a sensory based auditory processing deficit.
FIGURE 24-1 Auditory pathway.
Tactile System
The tactile system is the first system to function in-utero and is the largest of the sensory systems in the body. Touch is said to be our “first language.” It is the oldest and most primitive expressive channel and it dictates our experiences in this world. The tactile system is part of the somatosensory system and travels along with proprioception in the dorsal column.
The tactile sensory receptors cover the skin and epithelia, skeletal muscles, bones and joints, internal organs, and the cardiovascular system. The system reacts to diverse stimuli using different receptors: thermoreceptors, mechanoreceptors, and chemoreceptors. Transmission of information from the receptors passes via sensory nerves through the dorsal column medial lemniscal pathway and the anterolateral system (AL), then into the brain. Processing primarily occurs in the primary somatosensory area in the parietal lobe of the cerebral cortex.
The dorsal column medial lemniscal is associated with tactile discrimination or perception: detection of size, form, contour, texture, and movement across the skin. The AL pathway has receptors that respond to rough stimuli, which does not induce tissue damage such as rubbing, squeezing, or pinching. AL pathways project to regions of the brain responsible for arousal (reticular system), emotional tone (limbic system), and autonomic regulation (hypothalamus); therefore, tactile defensive behavior may exhibit behavior consistent with any of these systems (Fig. 24-2). Inadequacies in processing tactile input can lead to a difficult time with activities of daily living. The child may have difficulty manipulating small objects; thus, activities such as cutting, writing, and coloring may be an issue. Poor discrimination may lead to tactile defensive behavior with the child’s protective system working overtime because the child may regard many touch sensations as threatening. This may lead to a frequent or near constant state of “fight or flight” and sympathetic overdrive. The most well-known tactile sensory issue is that of tactile defensiveness. Tactile defensiveness among children can be one of the biggest dictators of a child’s behavior. These children can appear to have ADHD because they are always fidgeting and appear to be distracted when constantly trying to modulate incoming tactile information. Because they are hypersensitive to touch, these children may prefer to play alone; therefore, they may be seen as “loners.” The tactile system receives sensory information from receptor sites in the skin (baroreceptors), providing information about light touch, pressure, vibration, temperature, and pain.
TABLE 24.3
Signs of Sensory Underresponsivity
Auditory
Had little or no vocalizing or babbling as an infant
Often speaks in a loud voice and/or excessively
Likes excessively loud music, games, or TV
Does not respond to or had difficulty with verbal cues or to name being called
Has difficulty understanding or remembering what was said
Needs instructions repeated often, or will say, “What?” frequently
Talks self through a task, often out loud
Appears oblivious to certain sounds
Often disoriented/confused about where a sound is coming from
Olfactory
Fails to notice or ignores noxious odors
Excessively smells new objects, toys, people
Has difficulty discriminating unpleasant odors
May drink or eat things that are harmful/poisonous because they do not notice the noxious smell
Unable to identify smells from scratch ‘n sniff stickers
Tactile
May crave touch, needs to touch everything and everyone
May be self-abusive; pinching, biting, cutting, or head banging
Has a high pain tolerance
Likes to put objects in their mouth
Seeks out surfaces and textures that provide strong tactile feedback
Often is not aware of being touched/bumped unless done with extreme force or intensity
Often injures self; burns, cuts, bruises, etc., because harmful act does not register
May not be aware that hands or face are dirty or feel his/her nose running
Frequently and unknowingly hurts other children or pets while playing
Repeatedly touches surfaces or objects that are soothing (e.g., blanket)
Seeks out messy play
Enjoys/craves excessively spicy, sweet, sour, or salty foods
Taste
May eat inedible objects such as dirt, chalk, crayons (pica)
Prefers foods with intense flavor, i.e., excessively spicy, sweet, sour, or salty
Frequently chews on hair, shirt, or fingers
Constantly puts objects in mouth; even past the toddler years
Likes brushing teeth/vibrating toothbrushes and even trips to the dentist
Visual
Complains about “seeing double”
Writes at a slant (up or down hill) on a page
Difficulty copying
Fatigues easily with reading, writing, drawing, video games, etc.
Often loses his or her place while reading or doing math problems
Difficulty finding differences in pictures, words, symbols, or objects
Has a hard time seeing the “big picture”; i.e., focuses on the details or patterns within the picture
Difficulty with following and tracking objects with eyes
Difficulty judging spatial relationships in the environment; i.e., bumps into objects/people or missteps on curbs and stairs
Has difficulty telling the difference between similar printed letters or figures; e.g., p & q, b & d, + and x, or square and rectangle
Makes reversals in words or letters when copying, or reads words backwards; e.g., “was” for “saw” and “no” for “on” after first grade
Vestibular
Appears to be in constant motion, can’t seem to sit still
Loves to swing or spin; can do so for long periods
Craves fast movement; always running, jumping, hopping, etc. instead of walking
Loves fast-moving and spinning rides at amusement parks
When sitting must rock, shake legs, or move head
Likes jumping on furniture or trampolines, spinning in a swivel chair, or getting into upside-down positions
Tends to be a “thrill-seeker”; dangerous at times
Proprioception
Seeks out jumping, bumping, and crashing activities
Kicks feet on floor or chair while sitting at desk/table
Prefers tight clothing
Likes heavy blankets
Likes to be squeezed/hugged tightly
Clenches or grinds teeth
Likes to push, pinch, bump, or hit others
Likes to chew on things such as lip, straws, pencils, shirt collar/sleeve, etc.
Loves jumping off high structures/furniture
Frequently falls on floor intentionally
Loves “roughhousing” and tackling/wrestling games
FIGURE 24-2 The sensory tract: medial lemniscus.
Light Touch Contrary to what one might think, light touch is often the most upsetting touch to children with tactile processing issues. A soft touch—having his or her face cleaned or hair brushed, or the touch of grass or sand—may cause the child to become distressed. To a hypersensitive tactile child, these sensations may feel like he or she is being cut with a sharp piece of glass. Hypersensitive tactile children may be difficult for the doctor of chiropractic to adjust because of the child’s fear or dislike of tactile input. “Desensitizing” the child with tactile and vestibular input prior to the adjustment can be very helpful in obtaining an adjustment on these children. Tactile input that may be helpful for desensitizing can include stroking the body with soft or silky fabric, deep compression of limbs, massage with massage ball, or having the child play with toys of varying textures. Tactile input should be determined by what is tolerable to the child.
Deep Pressure Deep pressure can actually be calming to children with tactile and proprioceptive processing issues. Doing joint compression, big bear hugs, deep massage, and wrapping the child in heavy blankets all can be therapeutic. Deep pressure can be a good technique to try when a tactile and/or proprioceptive sensory child is having a meltdown.
Vibration Hypersensitive tactile children can be bothered by vibrations from cars or trucks on the road or an electric toothbrush, and act with a startle reaction when these situations occur. On the other hand, children that are hyposensitive actually enjoy vibratory sensation and think that sitting on the washer or dryer is great. For the hyposensitive child, using vibrating massagers, electric toothbrushes, and vibrating toys can be calming.
Temperature Some hyposensitive children will eat food that is so hot that it burns the inside of their mouth or leave their hand on a hot stove burner until it burns them, both of which will barely faze them. Tactile sensitive children can also be picky eaters. One reason for this is that they may not eat certain foods if the food is not at the particular temperature that they like.
Pain Some children may scream uncontrollably after a fall resulting in a small scrape whereas others may get up and “shake it off” but actually have a broken bone. Again, depending if the child is hypersensitive or hyposensitive, pain is very subjective as is temperature. For the tactile system to function properly, it relies on a balance between the following protective and discriminative capabilities:
Registration: the brain should register when there is a touch stimulus somewhere on the body.
Orientation: without looking, the child should be able to know the orientation/place where the stimulus is on their body.
Interpretation: without looking, the child should be able to interpret the sensation: hot, cold, sharp, dull, and interpret if it is dangerous/harmful or not.
Sensory modulation: after registration, orientation, and interpretation the child should be able to inhibit/screen out the stimulation and/or react appropriately to remove the stimulus.
In addition to a balance between protective and discriminative capabilities, there also needs to be a shift of importance from a defensive tactile system to a discriminative tactile system. As an infant, the defensive system is the most important because it alerts the caregiver that something is harmful. A baby cries when something is uncomfortable, alerting the caregiver that something may be wrong. During the toddler years, the defensive system and the discriminative system are equally important. This allows the toddler to start to become autonomous in the world but still alert the caregiver should there be something of potential danger touching him or her. By kindergarten, the discriminative system is the most important because by this age, the child should be less dependent on their caregiver. The child should be able to tell if there is danger with a particular stimulus that they may be in contact with, or potentially become in contact with, in order to avoid being harmed. Therefore, if a child age 5 or older continually presents with injuries such as cuts, burns, and bruises, one must not only rule out the possibility of child abuse but also of a poor discriminative and/or hyposensitive tactile system. Tables 24-2 and 24-3 show characteristics associated with sensory based tactile dysfunction.
Oral Tactile Hypersensitivity
One of the most difficult challenges in children with SPD can be the picky eater. Oral tactile hypersensitivities can greatly interfere with feeding as an infant and may cause the child to reject the nipple or new food textures as they get older because he or she is so sensitive to touch around the mouth. The breastfeeding mother can become very anxious when trying to feed an infant with hypersensitive oral tactile issues because the baby often pulls away from the breast or bottle and screams in distress. The child may also thrash his or her arms or legs in distress over the tactile contact to the mouth and/or body. The tactile contact around the infant’s mouth may feel like an electric shock to them. When picky eaters start to eat solid foods, the stress on the parents can be enormous as these children will generally have a very narrow range of foods that they will eat; often only two to three different items. They will generally either like crunchy/chewy type foods or soft/smooth textured foods. Children that prefer crunchy or chewy foods are generally seeking proprioceptive input as these foods allow them to bite and chew, which generates a great deal of proprioceptive feedback to the CNS.
To help avoid or to minimize the long-term and more complicated issues of oral tactile sensitivity, tactile stimulation around the mouth is important during infancy. The practitioner should suggest to the parents that they use various textures on the child’s face for tactile stimulation, especially around the mouth. Some suggestions to use for tactile stimulation are feathers, different fabrics, brushes, and various textured toys.
Taste System
Taste is a sensory function of the CNS. The receptor cells for taste in humans are found on the surface of the tongue, along the soft palate, and in the epithelium of the pharynx and epiglottis. Three cranial nerves are responsible for bringing the sensation(s) of taste to the brainstem.
Cranial nerve VII (facial) supplies taste to the anterior two-thirds of the tongue and is responsible for the sensation of sweet, sour, or salty.
Cranial nerve IX (glossopharyngeal) supplies taste to the posterior one-third of the tongue and is responsible for the sensation of bitterness.
Cranial nerve X (vagus) is responsible for a small area of sensation from the epiglottis.
The sensations of taste and smell are so interrelated that it can be difficult to distinguish which sensory system may be dysfunctional. This is especially difficult when it comes to food because so much of what we think is our taste is actually coming from smell. Many common characteristics associated with sensory based taste dysfunction are the same as those associated with sensory based olfactory dysfunction. Tables 24-2 and 24-3 list characteristics associated with sensory based taste disorders.
Olfactory System
Smells are detected by olfactory sensory neurons in the olfactory epithelium. Olfactory sensory neurons project axons to the brain within cranial nerve I (olfactory). These axons pass to the olfactory bulb, which in turn projects olfactory information to the olfactory cortex and other areas. The mitral cells leave the olfactory bulb in the lateral olfactory tract, which synapses on five major regions of the cerebrum: (a) the anterior olfactory nucleus, (b) the olfactory tubercle, (c) the amygdala, (d) the piriform cortex, and (e) the entorhinal cortex. The entorhinal cortex projects to the amygdala and is involved in emotional and autonomic responses to odor. It also projects to the hippocampus and limbic system and is involved in motivation and memory. No other sensory system has such strong connections to our feelings as does the olfactory system. This is most likely because there are projections that go to the limbic system, which is the core center of one’s emotions, memory, and learning.
Children with olfactory sensory-based dysfunction will often have allergies associated with chemicals, perfumes, lotions, cleaning products, etc. A parent may notice that their child’s behavior is “off the hook” or that he or she gets sick after being exposed to various chemicals. Many of these chemicals are petrochemicals that are volatile organic compounds and they off gas into the environment. When purchasing new furniture or a new mattress, parents should consider avoiding the fire-retardant or stain-resistant chemicals that are usually applied to these items. New paint and carpet can also be very harsh on these children; nonvolatile organic compound paints are the best choice for any environment and there are many brands available on the market. New carpeting not only has petrochemicals but also stain-resistant chemicals; parents should look for alternative “green” products, such as natural stone or bamboo, instead. A great and safe cleaning product for the home is the use of warm water and vinegar instead of the traditional harsh cleaning chemicals. These suggestions should also be taken into consideration in the chiropractor’s office, especially if the doctor is caring for the pediatric population. There are many books available on alternative “green” products to recommend for parents. Doctors may also make these materials available in their office lending library for easy access to parents. Tables 24-2 and 24-3 list characteristics associated with olfactory-based sensory disorders.
Visual System
First and foremost, it is important to understand that most children with visual processing disorder have 20/20 vision. Because visual processing skills are not closely correlated with acuity, a child who has 20/20 vision with excellent visual acuity can have deficient visual processing. Most people think that if a child’s vision is 20/20, then everything is fine. However, visual processing is more than just clarity; it also includes binocular coordination, speed accommodation, vertical movement, and other visual functions necessary to visualize, understand, and apply the information received. Children with visual processing dysfunction may have difficulty comprehending what they read, are unable to perceive spatial relations, or have difficulty with concentration. Thus, they seem easily distracted, which may be mistaken for ADD/ADHD. Below is a list of some general questions to screen children for possible visual processing dysfunction.
Does the child require a lot of time to complete homework?
Does the child complain of blurred vision or double vision, especially when reading?
Does the child complain of eye strain or headaches, especially when reading?
Does the child have difficulty copying?
Does the child lose his or her place or skip words or lines when reading?
Does the child reverse letters, numbers, or confuse similar words?
Does the child have difficulty with handwriting?
Tables 24-2 and 24-3 show characteristics of children with sensory-based visual processing dysfunction.
Visual Pathway
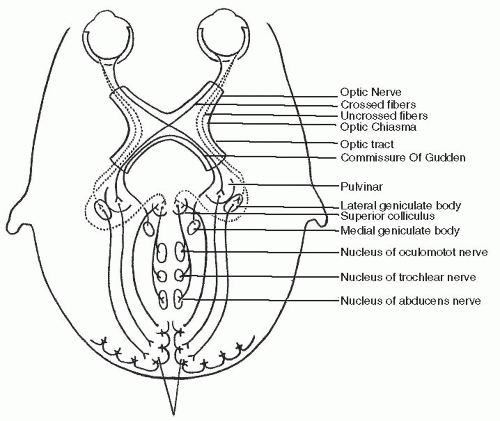
Information about a particular image via the eye is transmitted to the brain along the optic nerve. Fibers from the nasal portion of the retina cross the optic chiasm and join with fibers from the temporal portion of the retina of the opposite eye. The tract then projects to the lateral geniculate nucleus (LGN) of the thalamus. This allows each hemisphere to receive visual information from the contralateral half of the visual world. Approximately 90% of the axons in the optic nerve go to the LGN. Another population sends information to the SC in the midbrain, which assists in controlling eye movements, or saccades. Cells here respond to horizontal movement within the visual field. Other input to the SC comes from the visual cortex and the spinotectal tract which carries somatosensory information from the spinal cord and medulla. Projections from the SC then go to the oculomotor nuclei, thalamus, and spinal cord (tectospinal pathway). The SC plays a role in the visual coordination of posture and the control of eye movements (Fig. 24-3). The smallest visual pathway is the accessory optic tract, which sends projections to small accessory nuclei around the oculomotor nucleus, the medial vestibular nucleus, the LGN, and other regions of the thalamus. Efferents then project to the inferior olive, which sends fibers to the vestibular component of the cerebellum.
FIGURE 24-3 The visual pathway.
Visual processing is a dual system composed of magnocellular cells that originate in the peripheral retina and project to the LGN and then to the visual cortex. These are large cells concerned with general features of objects and object movement; they contribute to our understanding of where an object is in relation to our bodies and to other objects. This system also gives us information about movement, location, speed, size, and shape of objects. This system is also referred to as our spatial vision. Parvocellular cells are smaller cells but greater in number and originate in the central retina and also project to the LGN and then to the visual cortex. They convey information about the finer details of vision along with information pertaining to form and color. They contribute to our understanding of the what of an object so we can identify and remember the object. This system is also known as our object vision. The visual cortex is the most massive system in the human brain and is responsible for processing the visual image. The region that receives information directly from the LGN is called the primary visual cortex. There is some evidence that suggests the magnocellular system may be related to some forms of dyslexia. Autopsies of adults who had a history of dyslexia showed fewer magnocellular cells than adults without dyslexia (2). Some researchers (19,20,21) have suggested that there may be a subgroup of children with dyslexia that have a defect in some elementary visual functions served by the magnocellular system.
Binocular Vision
Binocular vision is when both eyes aim simultaneously at the same visual target. Both eyes must work together simultaneously, equally, and accurately as a coordinated team. Healthy binocular vision produces two important visual perceptual skills that are part of normal human vision: (a) binocular depth perception and (b) stereopsis, vision wherein two separate images from both eyes are successfully combined into one image in the brain. Extraocular proprioception is important for the normal development of binocularity and oculomotor control. Impaired extraocular proprioception may lead to latent nystagmus. Afferents from extraocular proprioceptors are from the ophthalmic branch of the cranial nerve V (trigeminal nerve) and the Gasserian ganglion to the spinal trigeminal nucleus and centrally from the ocular motor nerves. Efferent proprioceptive information is distributed to the SC, vestibular nuclei, nucleus prepositus hypoglossi, cerebellum, frontal eye fields, and visual cortex.
Binocular vision is extremely important for voluntary eye movements such as eye tracking and localization and is closely tied with the vestibular and proprioceptive systems. The vestibular system is responsible for holding the head in position so the eyes can focus on the intended target. In addition, proprioceptors within the cervical spine help to orientate the head and coordinate movements of the eyes, head, and neck to the task at hand. Therefore, proper functioning vestibular and proprioceptive systems are a vital part of processing visual information.
Convergence, divergence, and fixation are all part of binocularity and a healthy oculomotor system. Convergence is required when focusing on objects that are close. If the eyes have significant difficulty turning in to focus on an object, this is termed convergence insufficiency. If the eyes reflexively turn in too far and want to cross when looking at an object up close, this is termed convergence excess. It is suggested that convergence failure may provide a mechanical reason why some children struggle to read because convergence is a necessary precursor to visual tracking when performing close-up work. In a study by Pauc (22), 100 children, ages 4 to 15, with a primary diagnosis of either dyslexia, dyspraxia, ADD, ADHD, obsessive compulsive disorder, or Tourette’s syndrome who were attending a clinic primarily treating children with learning/behavioral disorders were selected. The children were tested for cerebellar function using the provoked Rhomberg’s test, the finger-to-nose test, dysdiadochokinesia of the upper extremities, and one-leg stand. Once assessed, the children were given specific cerebellar exercises to perform at home three times a day. The children with convergence failure were further tested using the visual therapy assessment program and then given the home therapy system program to do once a day. All children showed marked improvement when retested for cerebellar function. This coincides with reports of vergence failure in patients with cerebellar lesions and ablation studies in monkeys. Studies on monkeys suggest that specific areas of the cerebellum function in individual components of the vergence complex. Based on the study by Pauc (22), a high percentage of children have convergence insufficiency in association with the primary diagnosis of ADD (44.44%), ADHD (58.82%), dyslexia (60.87%), and dyspraxia (54.15%). Divergence is the ability to focus on an object at a distance or as it moves away from the body. When a child is reading in class and then must suddenly look up to focus on the teacher, the eyes should quickly adapt via divergence. Visual fixation is the ability to look at and focus on an object for a length of time. A newborn should be able to focus on large objects 8 to 10 in. from his or her face for few seconds. By 2 to 3 months of age, fixation should be fully developed, and by 5 to 6 years of age, a child should be able to fixate on an object 18 to 24 in. from his or her face for 10 seconds. If a child does not have the ability to fixate on objects, it is likely that he or she will have a difficult time academically, especially with reading and writing activities, as well as trouble with sports. If they cannot hold their eyes steady, the information they receive visually will be lost, distorted, and/or misunderstood. Other areas in which binocular vision may be dysfunctional include suppression, which is when the brain neglects the imagery coming in from one of the eyes, and diplopia. Characteristics that indicate possible problems with binocularity are:
Double vision
Difficulty with sports involving a ball
Difficulty with visually guided movements
Difficulty sustaining attention, especially with upclose tasks
Accommodation
Accommodation, or eye focusing, is the mechanism to focus the lens of the eye to obtain a high degree of visual acuity. It results from contraction or relaxation of the ciliary muscle and allows a shift of focus from a near point to a far point and vice versa. Accommodation changes with age; at about 4 months of age, children should begin to use both eyes together to track people and objects moving toward and away from them. By about 6 months of age, accommodation becomes more firmly established and continues to develop until it matures during the teenage years. Accommodation insufficiency is the inability or lack of skill or endurance for making close objects clear. Accommodation infacility is the inability to fluently and effortlessly focus from far to near and back.
Visual accommodation is the result of a fine balance between the parasympathetic and sympathetic nervous system. Parasympathetic fibers begin in the Edinger-Westphal nucleus of cranial nerve III (oculomotor) and excite the ciliary muscle for pupillary constriction, which helps focus on objects that are close. Sympathetic fibers begin at the intermediolateral horn cells of spinal cord levels C8-T4 and ascend in the sympathetic chain. They then synapse in the superior cervical sympathetic ganglion, travel with the carotid artery, and supply innervation of the ciliary muscle to flatten the lens of the eye. The sympathetic fibers are responsible for pupillary dilation and focusing the eye on distant objects (23). Therefore, if injury is sustained to the cervical and/or upper thoracic spine, such as is the case with whiplash, compromise of the sympathetic innervation to the eye can occur. As stated early in the chapter, breech deliveries can cause damage to the lower cervical and upper thoracic spine; thus, one must consider possible accommodation issues in children that presented at birth in the breech position. Accommodation disturbances have been cited as one of the causes of visual disturbances following whiplash injury. In a 2003 study, Brown (24) studied a group of 19 whiplash subjects and a control group of 43 subjects; he found that there was reduced amplitude of accommodation in the whiplash group subjects compared to the control group subjects. These results indicate that whiplash was associated with defective accommodation in that particular select group of whiplash subjects. Various ocular effects have been reported in the literature in regards to spinal manipulation therapy. Changes in visual acuity, oculomotor function, intraocular pressure, and pupillary size are some of the major changes reported. In a literature review, Gorman, an ophthalmologist, and Terrett, a chiropractor, reviewed 12 journal articles from 1964 to 1992 describing the experiences of 187 patients with visual changes after cervical spine care (25). Conditions included in this study were blurred vision; decreased vision; contraction of visual fields; oculomotor dysfunctions (diplopia, nystagmus, visual fatigue, etc.); pupillary changes; ptosis; eye pains; dry eye; tearing eye;, distention of eye; as well as others. Interestingly, Gorman and Terrett (25) believed that the improved vision and eye conditions were merely side effects of overall improved brain function from the chiropractic adjustments. The following are some characteristics of accommodation dysfunction:
Inattention, especially for near work
Difficulty copying
Blurred close-up focus
Headaches from visual work
Eye pain/strain from visual work
Requiring a long time to do homework
Visual-Motor Integration
Visual-motor integration refers to the ability to coordinate a visual stimulus with fine and gross motor movement. This system is regulated by vestibular, proprioceptive, and tactile feedback loops. A child with difficulty in this area has problems coordinating what he or she see with an appropriate motor response required in fine motor skills such as copying, or in gross motor skills such as kicking a football or shooting a ball into a basket. When learning any new skill, one initially uses his or her eyes to help guide the arms, legs, hands, and feet. For example, when learning how to roller skate, children will initially use their eyes to watch and guide their feet. When learning a musical instrument or learning the computer keyboard, they will watch their fingers. Once the proprioceptive and vestibular systems take over, these motor tasks should become automatic and the eyes can look at other objects or at their surrounding environment. However, if either the vestibular and/or proprioceptive system(s) are deficient, the child will compensate by using vision to carry tasks that should be “automatic.” The child may become frustrated because tasks that should be automatic are difficult and awkward; therefore, the child just gives up. Behaviors consistent with visual-motor integration dysfunction include:
Poor motor responses to visual stimulation: difficulty with sports, often does not participate
Poor handwriting: speed and/or accuracy
Poor drawing/copying
Visual Perception
Visual perception is the ability to interpret information from visible light reaching the eyes that is then made available for planning and action. Some children suffering from developmental disorders, learning disorders, and autism have a form of visual perceptual disorder called scotopic sensitivity disorder, also known as Irlen Syndrome. This disorder is said to primarily affect reading- and writing-based activities and is caused by hypersensitivity to lights, patterns, glare, contrast, and colors. Scotopic sensitivity syndrome is based on the theory that some individuals have hypersensitive photoreceptors, visual pathways, and/or brain systems that react inappropriately to physical energy (wavelengths). Vision occurs when energy is received by the retina’s photoreceptors, initiating a biochemical process affecting the visual pathways and deep structures of the brain. This disorder is estimated to affect more than 10% of the general population and nearly half of the autistic population (26).
Part of visual perception is laterality—knowing one’s own midline, left, and right sides. Children with poor laterality may have trouble with crossing the midline activities. In severe cases, children may even seem to “ignore” one side of their body as if they do not realize that they have a right or left side. Children that have issues with laterality may have trouble academically with reading and writing, as these require crossing the midline. A child may also have a visual perceptual midline shift. This is when the perceived midline of the body is no longer actually at midline. Therefore, a target that is actually at the midline of the body will be perceived to be either to the child’s right, left, or higher or lower. Children with a midline shift may constantly bump into objects, trip forwards or fall backwards, or have inaccurate eye-hand or eye-body movements.
Directionality is also a part of visual perception and involves the concept of projecting laterality into the spatial environment ultimately to develop an organized understanding of the positional relationships of objects in space, as referenced to the individual, in the X, Y, and Z axes. Other parts of the visual perception system are:
Visual discrimination: the ability to see subtle distinctions among similar objects
Visual spatial relations: the ability to see that an object has been reversed, usually to its mirror image
Visual closure: the ability to see what an object would be even though the visual information that would completely represent the entire form is missing
Visual memory: the ability to recall the visual image of an object previously seen without using sounds or symbols to support the image
Visual sequential memory: the ability to recall the sequence of objects without the use of sounds or symbols to support the sequence
Visual figure-ground: the ability to separate the desired object from the rest of the information in the viewing field
Characteristics that are associated with visual perception dysfunction are:
Difficulty understanding what is being seen
Difficulty remembering what is seen
Difficulty matching what was seen with what is already known
Difficulty with reading comprehension
Difficulty with creativity
Difficulty with orientation
Visual Hypersensitivity
Children may have trouble screening out visual input and seem to be not paying attention because their eyes are constantly going from one target to another. With a world full of visual input, it is necessary that children be able to filter out what is and what is not visually important. For example, a child may be in a classroom visually moving his or her attention from the teacher, to a fly, to something passing by the window, to another child scratching his head, to what is written on the white board, etc., and all the while he or she should be trying to learn. Such is the case when a child has difficulty directing his or her visual attention to one area because he or she is distracted by conflicting visual stimuli and/or because he or she is unable to fixate visually on an object. If people are only able to fixate visually for a split second, they may only get a fraction of the material presented to them and they will not have all of the information necessary to interpret and process the whole of what is seen. Anytime a child shifts his or her focus, then he or she must also change his or her accommodation depending on the distance of the stimuli. Therefore, fixation and accommodation work closely together. On the other hand, children may hyperfocus on visual stimuli and appear transfixed and as though they are gaining nothing from the activity; however, they are tuning everything else out so that they can process the visual stimuli. Tables 24-2 and 24-3 show characteristics of sensory-based visual disorder.
Vestibular System
The vestibular system is in place at 8 weeks’ gestation, is functional at 16 weeks, and should be fully developed by 6 months after conception. It is myelinated at the time of birth and it is the only sensory system to be mature at the time of birth with both efferent and afferent cerebellar linkages. In-utero, the fetus receives constant vestibular stimulation from movement of the amniotic fluid and the movement of their body as well as the mother’s own body movement. This is an important consideration for the doctor of chiropractic because in-utero constraint caused by maternal pelvic subluxations may interfere with fetal movement.
The vestibular system must learn to interact with all of the other sensory systems within the first months of life. It is considered the most important of the sensory systems as it has the most influence on the other sensory systems and on a person’s ability to function in everyday life. It also acts as the “volume control” of all sensory information received and will inhibit or facilitate all incoming sensory information. When there are weak or inconsistent neural connections between the vestibular system and any one or more of the other sensory systems, the sensory information received will not be reliable and the child will have sensory processing dysfunction. The vestibular system acts as the “conductor of the orchestra,” telling each sensory system when and where it should go or stop and at what volume. It informs the CNS where it is in relation to the pull of gravity for an individual to maintain his or her balance and equilibrium. This system has a strong impact on developmental motor skills, visual-spatial and language skills, hand dominance, reading, writing, and motor planning. The most common vestibular-based disorders are listed in Table 24-4.
TABLE 24.4
Vestibular-Based Disorders
Gravitational insecurity
Arousal
Vestibular hypersensitivity
Vestibular hyposensitivity
Vestibular-visual integration disorder
Vestibular-proprioceptive integration disorder
Bilateral integration and sequencing disorder
Vestibular Labyrinth
The vestibular labyrinth lies in the petrous portion of the temporal bone and is part of the peripheral vestibular system. It consists of three semicircular canals that are sensitive to angular accelerations (head rotation) and two otoliths that are sensitive to linear accelerations (straight-line). The otolith organs are composed of the utricle, which senses motion in the horizontal plane (forward-backward, left-right, or combination) and the saccule, which senses motion in the sagittal plane (up-down movement) (Fig. 24-4). Vestibular receptors are hair cells located in the otolith organs and in swellings at the base of the three semicircular canals. At the base of each hair cell lies the afferent process of the vestibular nerve. In addition to the afferent fibers there are also efferent fibers that originate in the vestibular nuclei and provide inhibitory control of the transmission of information from the hair cells and can prevent information from traveling beyond the receptor site. With a unilateral lesion or deficit, the right and left labyrinth becomes disordered, resulting in a decreased firing rate of the vestibular nuclei on one side. A unilateral lesion affects the system as if the intact side were being stimulated, thus generating an illusion of change in head position and movement. The disequilibrium then activates the vestibulospinal system to respond inappropriately, resulting in vertigo, nystagmus, and postural instability.
FIGURE 24-4 Vestibular labyrinth.
Vestibular Nerve and Nuclei
The cell bodies for the vestibular nerve are located in Scarpa’s ganglion. From the cell bodies, the vestibular nerve carries information to the four vestibular nuclei in the brainstem: the lateral vestibular nucleus, the medial vestibular nucleus, the superior vestibular nucleus, and the inferior vestibular nucleus. The vestibular nerve sends projections both ipsilaterally and contralaterally. The nuclei can determine direction of movement by comparing the frequency of impulse flow between the right and left canals and otolith organs. There are extensive connections between the vestibular nuclear complex, cerebellum, oculomotor nuclei, brainstem RAS, thalamus, cortex (frontal lobe or anterior portion of the parietal lobe) and spinal cord. The lateral vestibular nuclei—Deiters’ nucleus—gives rise to the lateral vestibulospinal tract, which projects ipsilaterally to all levels of the spinal cord but is most abundant in the cervical and lumbosacral enlargements (Fig. 24-5). It is of prime importance in regulating muscle tone so that balance is maintained and it has a strong influence on postural muscles, postural control, and stability. The medial, superior, and inferior vestibular nuclei give rise to the medial vestibulospinal tract, which only descends to the cervical segments. The medial vestibulospinal tract is the caudal extension of the medial longitudinal fasciculus that controls eye movement (Fig. 24-6). This tract receives input from the cerebellum and skin and joint proprioceptors. It assists with the maintenance of consistent position of the head in space (equilibrium) and its descending vestibular projections interact with proprioceptive input from the cervical spine. Ascending fibers of the medial longitudinal fasciculus, some cross and some uncrossed, connect the vestibular nuclei with the nuclei of the abducens, trochlear, and oculomotor nerves, and with the accessory oculomotor nuclei of the midbrain. It provides for conjugate movement of the eyes, coordinated with movement of the head, to maintain visual fixation. The medial vestibular nucleus is the largest of the nuclei and is closest to the midline. It sends crossed fibers to both the extraocular nerve nuclei and to the cerebellum and it also sends most of the fibers to the medial vestibulospinal tract. The superior vestibular nucleus sends uncrossed fibers to cranial nerves III and IV. The inferior vestibular nucleus integrates input from the vestibular system and the fastigial nucleus of the cerebellum.
FIGURE 24-5 Lateral vestibulospinal tract. Cells of origin are from the lateral vestibular nucleus. The pathway is uncrossed and courses the entire length of the spinal cord; located in the ventral funiculus. The pathway enables the vestibular apparatus to influence the ipsilateral proximal limb muscles.
Vestibular-Visual and Vestibular-Proprioceptive Integration
The vestibular system sends signals primarily to the neural structures that control our eye movements and to the muscles that keep us upright. The projections to the former provide the anatomical basis of the VOR, which is required for clear vision. In conjunction with the visual and proprioceptive systems, the vestibular system lets us know if we are right side up, upside down, or lying down. The visual and vestibular systems interact primarily through a series of reflexes and tracts, namely the VOR, the vestibulospinal tract, and the dorsal and ventral spinocerebellar tracts. For a child with weak visual-vestibular integration, it can be very frightening when they hang upside down because it is as though the whole world has flipped. They may be able to handle tasks in which the head is fairly steady, such as reading; however, when they participate in an activity or sport that requires head/body movement along with vision, they may not perform well. An example of this is the child who, when walking, often bumps into people, doors, or furniture. Vestibular-proprioceptive integration is responsible for muscle tone and posture, giving muscles the information they need to contract and stay upright and move against gravity. It is thought that vestibular and proprioceptive processing work jointly to contribute to the perception of active movement; the development of body schema; and the development and use of postural responses, especially those involving the extensor muscles. Static muscle control or cocontraction is also a part of vestibular-proprioceptive integration. A child who has a deficit in vestibular and/or proprioceptive functioning will have difficulty contracting muscle groups that surround a joint for stability. He or she may have trouble just standing still because this requires the muscle groups surrounding the hips, knees, and ankles to be in a state of cocontraction. A child with poor static muscle control will appear as though he or she is in constant motion because it is almost impossible for them to be still.
FIGURE 24-6 Medial vestibulospinal tract. Cells of origin are from the medial vestibular nucleus. The pathway is bilateral but the ipsilateral projection is more dense. The pathway innervates the cervical and upper thoracic spinal cord and influences mainly the neck and axial muscles.
Only gold members can continue reading. Log In or Register to continue