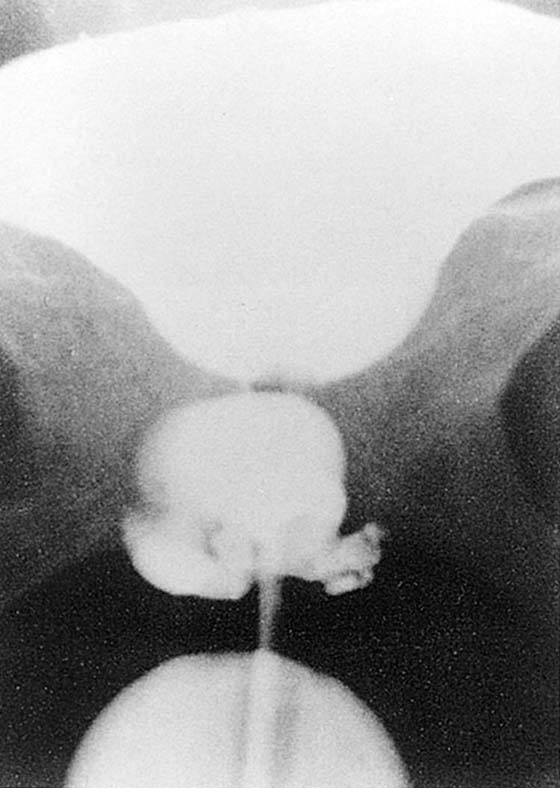
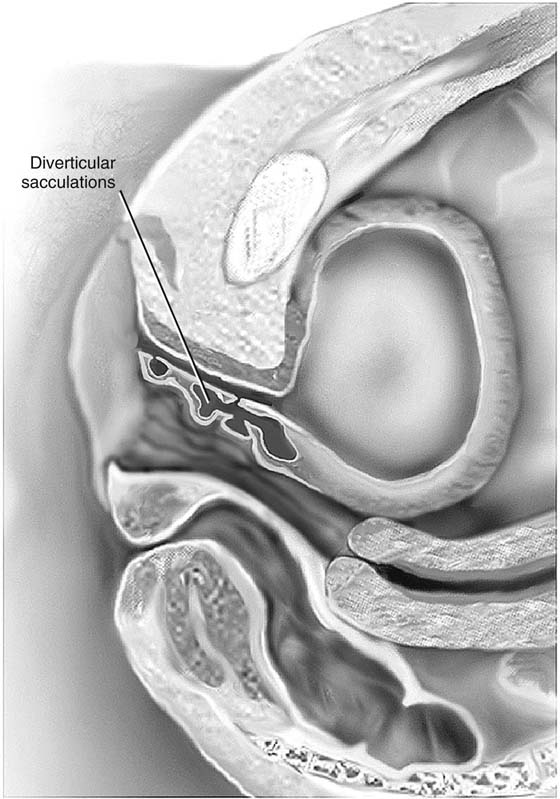
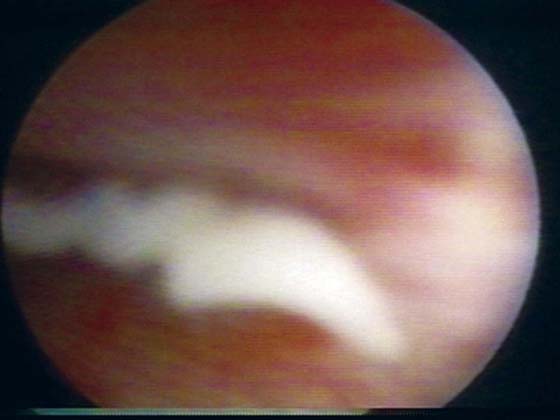
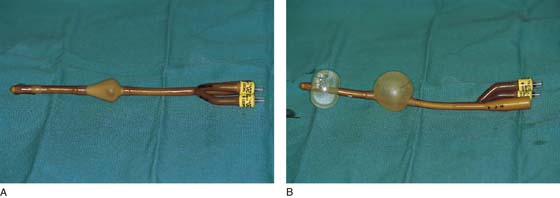
CHAPTER 84 For practical purposes, a suburethral diverticulum is any fluid-filled mass along the anterior lateral portions of the vagina that can be shown to have a direct communication with the urethra. Patients with a suburethral diverticulum may be asymptomatic or may complain of chronic recurrent cystitis, pain, burning and frequency, dyspareunia, voiding difficulty, postvoid dribbling, urinary incontinence, gross hematuria, or protrusion of a vaginal mass. Surgery should be considered only when the diverticulum becomes symptomatic. A Tratner double balloon catheter (Fig. 84–1A, B) is specially designed to assist in the diagnosis of a diverticulum, as well as in the identification and location of the diverticulum at the time of surgery. The catheter is composed of a proximal balloon that inflates within the bladder neck, anchoring the catheter, and a distal balloon that occludes the external meatus (see Fig. 84–1B). Contrast fills the urethra through a slit between the balloons. With this catheter, the urethra basically becomes a closed tube that can be injected with contrast medium under moderate pressure, permitting radiographic visualization of diverticula even with minute sinus tracts. This has been termed positive-pressure urethrography (Fig. 84–2). The degree of difficulty associated with repair of diverticula depends on their size and number (Fig. 84–3), the position of the ostium in relation to the bladder neck and trigone, and the degree of inflammation. Very commonly pus or discharge can be seen at the urethral meatus (Fig. 84–4) or in the urethra (Fig. 84–5) when anterior vaginal wall massage is performed. Large multiloculated or saddle-shaped diverticula in the proximal urethra or bladder neck region may require extensive dissection extending under the trigone (see Fig. 84–3). In these situations, preoperative placement of ureteral stents may facilitate identification of ureters and reduce the risk of damage during dissection. Some surgeons will routinely perform a suburethral sling at the time of repair of a diverticulum if they believe that the incontinence mechanism is going to be significantly compromised. In these situations, transposition of the labial fat pad between the repaired diverticulum and the suburethral sling should be performed (see Chapter 85, Martius Fat Pad Transposition and Urethral Reconstruction). FIGURE 84–1 Tratner double balloon catheter. A. Note the deflated proximal and distal balloons. B. Inflation of the proximal and distal balloons makes the urethra a closed tube that could be injected with contrast medium under moderate pressure, permitting radiographic visualization of diverticula even with minute sinus tracts. FIGURE 84–2 Positive-pressure urethrogram showing a large, multiloculated suburethral diverticulum. (From Walters MD, Karram MM: In Urogynecology and Reconstructive Pelvic Surgery, 2nd ed. CV Mosby, St Louis, 1999, with permission.) FIGURE 84–3 The varied potential complexity of urethral diverticula. Note the small distal diverticulum, which if symptomatic could be treated with a Spence procedure, in contrast to a complex multiloculated proximal diverticulum. FIGURE 84–4 Anterior vaginal wall massage in a patient with an infected diverticulum produces a discharge from the urethral meatus. FIGURE 84–5 Urethroscopic view of diverticular opening. Note that puslike discharge is seen exiting the opening when anterior vaginal wall massage is performed. Multiple methods have been described to surgically correct the suburethral diverticulum. The two most commonly performed techniques are diverticulectomy and the partial ablation technique. With both techniques, a “vest-over-pants” closure of the periurethral fascia is utilized to avoid overlapping sutures and thereby reduce the incidence of urethrovaginal fistula (Figs. 85–6 through 85–8). Following is a step-by-step description of the techniques utilized to repair a urethral diverticulum: 1.
Repair of Suburethral Diverticulum
![]()
Stay updated, free articles. Join our Telegram channel


Full access? Get Clinical Tree


