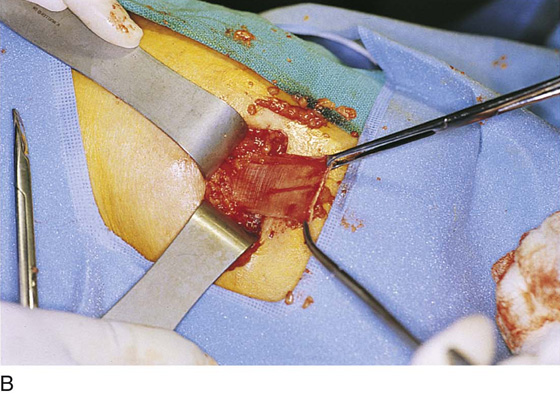
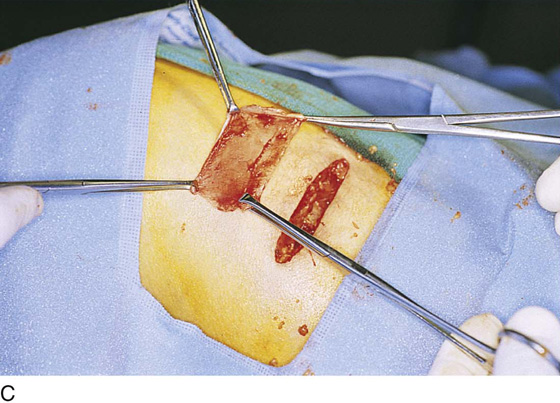
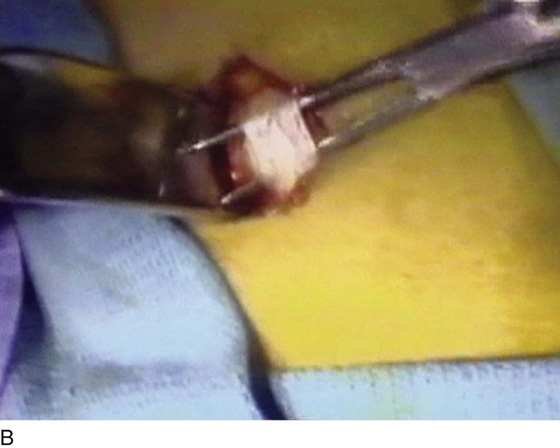
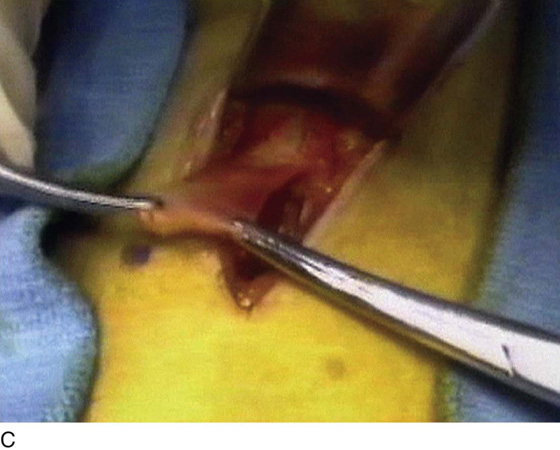
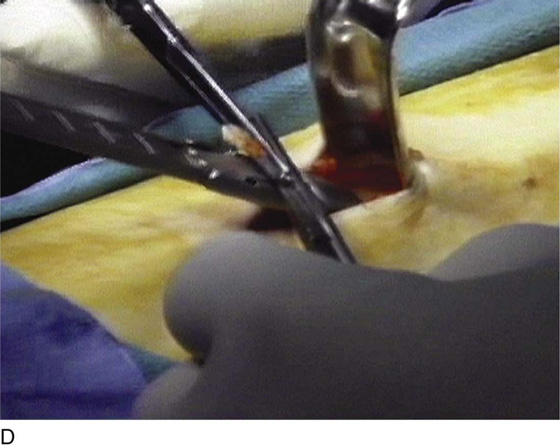
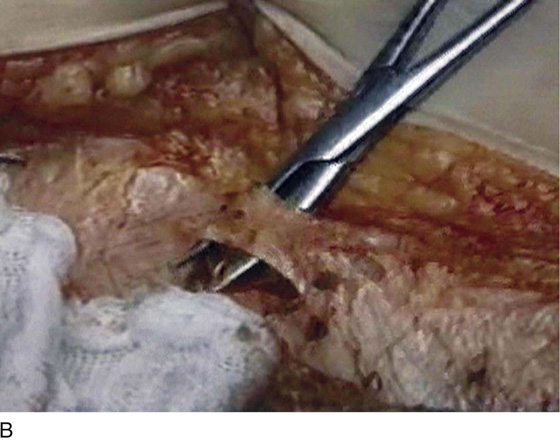
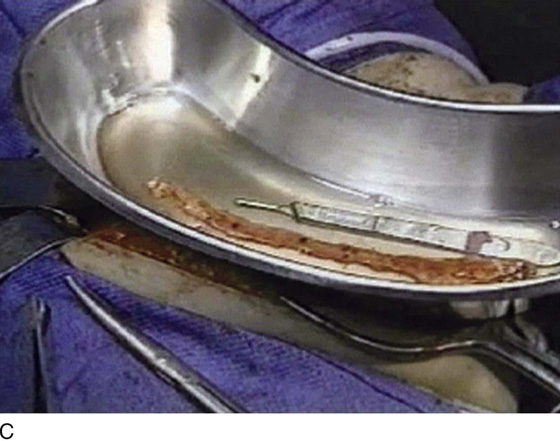
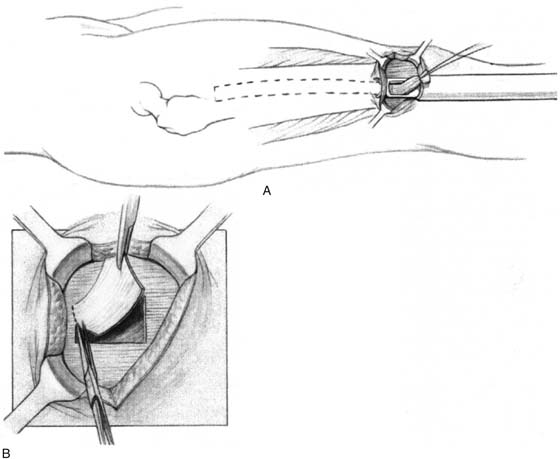
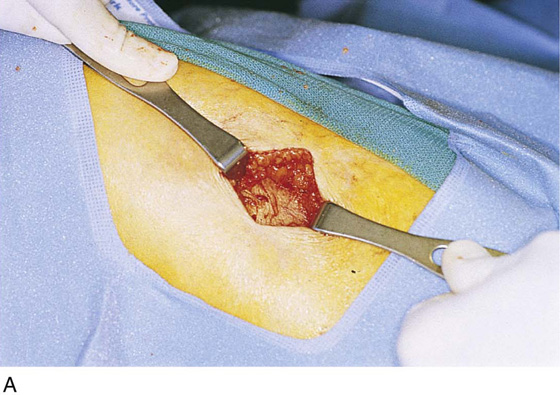
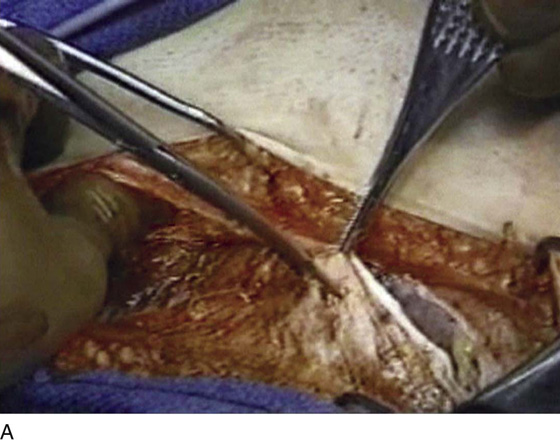
CHAPTER 59 Mickey M. Karram Pubovaginal slings are well-accepted procedures utilized for the correction of stress incontinence. Materials utilized for pubovaginal slings are always biologic and are placed at the proximal urethra and bladder neck. Currently used biologic materials are divided into autologous tissue, which is harvested from the patient who is undergoing the sling; allograft material, which is most commonly cadaveric fascia lata; and xenografts, which are harvested from various animal sources. Technically, bladder neck slings are called pubovaginal slings when the arms of the material used are connected to the anterior rectus fascia on each side. Various modifications of a traditional pubovaginal sling have been described and involve various patch-type slings in which the sling materials are placed vaginally at the level of the proximal urethra and then are attached to sutures that are passed suprapubically. Proximal suburethral slings work best when bladder neck mobility and vaginal pliability are present. Although plenty of data are available to support the use of pubovaginal slings as a primary operation, these procedures are usually reserved for patients who have failed synthetic midurethral slings, or who have a contraindication for the use of a synthetic material. If the surgeon decides to utilize autologous tissue, this will most commonly be fascia lata or rectus fascia. Harvesting of these tissues usually will occur before any vaginal dissection is performed. The technique used to harvest fascia lata is determined by whether the surgeon prefers to do a complete pubovaginal sling, in which the fascia will need to extend from the anterior abdominal fascia to below the proximal urethra and back to the anterior abdominal fascia on the opposite side, or if the surgeon prefers to place a patch-type sling. If a patch-type sling is used, a patch of rectus fascia or fascia lata is harvested. To harvest a patch of fascia lata, a 3- to 4-cm transverse skin incision is made about 8 cm above the midpatella lateral to the knee and the lower thigh. Blunt dissection exposes the underlying fascia lata. A 4 × 6-cm piece of fascia lata is removed and will serve as the patch for the sling procedure (Figs. 59–1 and 59–2). Subcutaneous tissue is reapproximated, the skin is closed, and a pressure bandage is placed. If a full pubovaginal sling is to be utilized, then a long piece of fascia lata can be obtained by using a Wilson or Crawford fascial stripper. The technique used to obtain a full strip of fascia involves a similar incision as described with the patch technique; however, fat is bluntly dissected away from the fascia lata, all the way up the lateral side of the leg toward the greater trochanter. A 1-cm-wide piece of fascia is then removed with the fascial stripper. This usually will produce a 20-cm-long piece of fascia. A second piece of fascia lata of similar length can be obtained by repeating the same procedure. A 1-cm-wide bridge of fascia lata should remain between the two areas where the stripper has removed the tissue (Fig. 59–3). These two pieces of fascia can then be sutured to each other, thus providing a 30- to 35-cm-long piece of fascia for use in providing the pubovaginal sling. If the rectus fascia is used for a pubovaginal sling, a transverse abdominal incision is made, usually 4 cm above the pubic symphysis. Blunt dissection is performed until the underlying rectus fascia is identified. Via a transverse incision in the fascia, a 1- to 2-cm-wide strip of fascia is sharply dissected away. If the goal is to have the arms extend to the anterior abdominal wall, then a 20-cm-long piece of fascia is harvested (Fig. 59–4). If a patch sling is to be placed, then a 2 × 8 piece of fascia is harvested. FIGURE 59–1 A. Technique for obtaining a strip of fascia lata using a vein stripper. B. Technique for obtaining a patch of fascia lata. Fascia lata patch has been excised. FIGURE 59–2 A. An incision on the lower leg is made about 8 cm above the midpatella lateral to the knee, exposing fascia lata. B. A patch of fascia is being excised. C. A fascia lata patch has been excised. FIGURE 59–3 A. Appropriate positioning of the leg for obtaining a full-length fascia lata strip. B. Exposure of a 1-cm-wide piece of fascia lata. C. Initial mobilization of a 1-cm fascial strip. D. Stripper is applied to the fascia lata to complete fascial stripping. E. Full-length strip of fascia lata. (Photographs A–D compliments of Dr Alfred Bent.) FIGURE 59–4 A. Rectus fascia has been exposed via a low transverse skin incision. B. A 1-cm-wide piece of fascia lata is exposed at the midline. C. Full-length piece of rectus fascia has been completely excised. (Photographs compliments of Dr Jerry Blaivas.)
Pubovaginal Slings for the Correction of Stress Incontinence
 Mark D. Walters
Mark D. Walters


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


