CHAPTER 6 Proper care in positioning patients for cervical, vulvar, vaginal, anal, uterine, and endoscopic surgery is of vital interest for the gynecologic surgeon. The dorsal lithotomy position regardless of whether it is implemented with a candy cane or Allen, or knee-crutch leg supports remains an unnatural state Figs. 6–1 through 6–3. When lithotomy position is coupled with the Trendelenburg position, additive abnormalities may ensue. Improper positioning can and will result in neurologic injury. Table 6–1 illustrates the frequency, causative factor(s), and specific locations of nerve injuries associated with obstetric and gynecologic surgery. The proper lithotomy position includes thighs and legs gently flexed; ankles and feet evenly supported; and avoidance of dorsiflexion of the foot, minimal abduction at the hip, buttocks firmly seated on the operating table, avoidance of overhanging buttocks, and knees (lateral) free from contact with leg support devices. Several lithotomy positions are acceptable. A low lithotomy position is quite satisfactory for dilation and curettage, hysteroscopy, and cystoscopy (see Fig. 6–1). A mid to high lithotomy position provides the best exposure for vulvar and vaginal surgery (Fig. 6–4). Although Allen leg supports are satisfactory for laparoscopic procedures, they are not advantageous or for that matter desirable for most vulvar and vaginal procedures. They may be indicated for radical vulvectomy surgery. FIGURE 6–1 This patient illustrates the low lithotomy position. Her legs are suspended in candy cane supports. FIGURE 6–2 This leg support incorporates a gel padding to protect the legs and feet. FIGURE 6–3 The Trendelenburg (head-down) position adds to the risk of nerve injury when the patient is in the lithotomy position. The inferior extremities are further deprived of blood flow. FIGURE 6–4 The high lithotomy position requires that the legs are flexed at the knee. Extension at the knee joint adds to the risk of sciatic or lumbosacral trunk injury. Hyperflexion at the hip will render the patient susceptible to femoral nerve injury (Fig. 6–5). The mechanism of injury relates to the fact that the rigid inguinal ligament compresses the femoral nerve trunk as the latter passes beneath it in its course from the abdomen into the thigh. Hyperextension at the knee joint and hip can produce stretch injuries to the lumbosacral trunk and/or sciatic nerve. Short periods of leg extension with the feet in candy cane supports are tolerable, but after 30 minutes, the risk of injury is increased. Excessive abduction (>45°) over 2 hours will endanger the obturator, genital femoral, and/or femoral nerves (Fig. 6–6). The latter nerve is particularly vulnerable when external rotation is added to abduction >45°. Compression at the head of the fibula will injure the peroneal division (Fig. 6–7) of the sciatic nerve, leading to paresis and pain in the leg following distribution of that nerve. Other causes of neuropathies associated with gynecologic surgery in patients who are not in the lithotomy position include self-retaining abdominal retractors, radical surgery, compression related to tight and prolonged packing, hematomas, tumors, and direct injury (e.g., incising the nerve). Figure 6–8A, B shows the key nerves and plexuses that supply innervation to the pelvis and inferior extremities. The relationships of the large nerve roots and trunks to the bony pelvis and to the ligamentous structures are detailed in the drawing. The largest nerves include (1) the sciatic nerve, which lies deep within the pelvis and exits the pelvis via the greater sciatic foramen (the nerve is in close proximity to the ischial spine and sacrospinous ligament [Fig. 6–9]); (2) the lumbosacral trunk, which contains elements of the lumbar and sacral plexuses and lies on the sacroiliac joint; and (3) the femoral nerve, which is embedded within the psoas major muscle. The nerve is exposed as it crosses beneath the inguinal ligament and exits via a groove between the iliacus muscle and the psoas major muscle (iliopsoas). After draping, it is wise to change the position of the suspended inferior extremities when surgery extends beyond 2 hours. Additionally, relief of pressure from retractor blades should be carried out every hour or two. Care must be taken with assistants leaning or resting on a patient’s inferior extremities in the lithotomy position (Fig. 6–10
Positioning and Nerve Injury
Positioning the Patient



Peripheral Nerve Injury
![]()
Stay updated, free articles. Join our Telegram channel

 Nerve Injuries Associated With Positioning and Pelvic Surgery
Nerve Injuries Associated With Positioning and Pelvic Surgery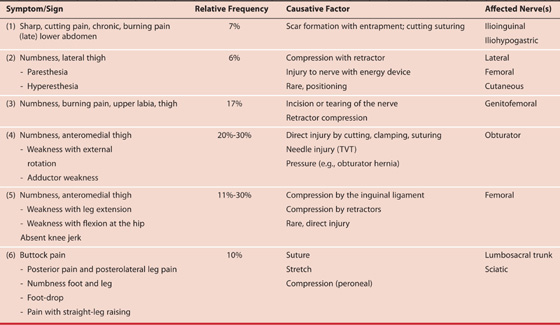

Full access? Get Clinical Tree


