Polycythemia
Deirdre O’Reilly
As the central venous hematocrit rises, there is increased viscosity and decreased blood flow. When the hematocrit increases to >60%, there is decreased oxygen delivery (1) (see Figure 46.1). Newborns have larger, irregularly shaped red blood cells (RBC) with different membrane characteristics than the RBCs of adults (1, 2, 3). As viscosity increases, there is impairment of tissue oxygenation and decreased glucose in plasma, leading to increased risk of microthrombus formation. If these events occur in the cerebral cortex, kidneys, or adrenal glands, significant damage may result. Hypoxia and acidosis increase viscosity and deformity further. Poor perfusion increases the possibility of thrombosis.
I. DEFINITIONS
A. Polycythemia is defined as venous hematocrit of at least 65% (2, 3). Hematocrit measurements vary greatly with site of sample, and capillary hematocrit may be up to 20% higher than venous (2). Hematocrit initially rises after birth from placental transfer of RBCs, then decreases to baseline by approximately 24 hours (4). The mean venous hematocrit of term infants is 53% in cord blood, 60% at 2 hours of age, 57% at 6 hours of age, and 52% at 12 to 18 hours of age (2).
B. Hyperviscosity is defined as viscosity >2 standard deviations greater than the mean (3). Blood viscosity, as described by Poiseuille, is the ratio of shear stress to shear rate and is dependent on such factors as the pressure gradient along the vessel, radius, length, and flow (4). The relationship between hematocrit and viscosity is nearly linear below a hematocrit of 60%, but viscosity increases exponentially at a hematocrit of 70% or greater (Figure 46.1) (4, 5).
II. INCIDENCE.
III. CAUSES OF POLYCYTHEMIA
Placental red cell transfusion
Delayed cord clamping may occur either intentionally or in unattended deliveries.
When the cord is clamped within 1 minute after birth, the blood volume of the infant is approximately 80 mL/kg.
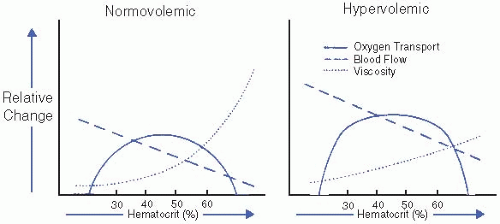
Figure 46.1. Effect of hematocrit on viscosity, blood flow, and oxygen transport. (Adapted from Glader B, Naiman JL. Erythrocyte disorders in infancy. In: Taeusch HW, Ballard RA, Avery ME, eds. Diseases of the Newborn. Philadelphia: WB Saunders; 1991.)
When the cord is clamped 2 minutes after delivery, the blood volume of the infant is 90 mL/kg.
In newborns with polycythemia, blood volume per kilogram of body weight varies inversely in relation to birth weight (see Figure 46.2).
Cord stripping (thereby pushing more blood into the infant).
Holding the baby below the mother at delivery.
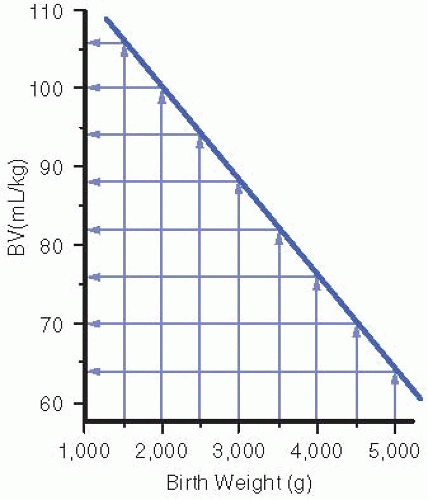
Figure 46.2. Nomogram designed for clinical use, correlating blood volume per kilogram with birth weight in polycythemic neonates; BV = blood volume. (From Rawlings JS, Pettett G, Wiswell T, et al. Estimated blood volumes in polycythemic neonates as a function of birth weight. J Pediatr 1982;101[4]:594-599.)
Maternal-to-fetal transfusion
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


