Fluid and Electrolyte Management
Fluid and Electrolyte Management
Careful fluid and electrolyte management in term and preterm infants is an essential component of neonatal care. Developmental changes in body composition in conjunction with functional changes in skin, renal, and neuroendocrine systems account for the fluid balance challenges faced by neonatologists on a daily basis. Fluid management requires the understanding of several physiologic principles.
I. DISTRIBUTION OF BODY WATER
General principles. Transition from fetal to newborn life is associated with major changes in water and electrolyte homeostatic control. Before birth, the fetus has constant supply of water and electrolytes from the mother across the placenta. After birth, the newborn assumes responsibility for its own fluid and electrolyte homeostasis. The body composition of the fetus changes during gestation with a smaller proportion of body weight being composed of water as gestation progresses.
Definitions
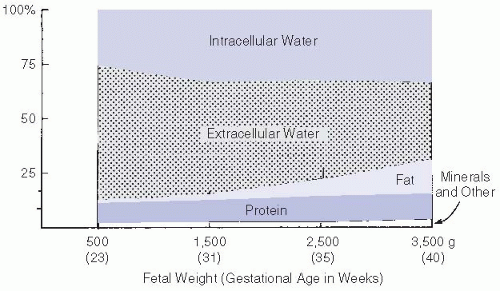
Perinatal changes in TBW. A proportion of diuresis in both term and preterm infants during the first days of life should be regarded as physiologic. This diuresis results in a weight loss of 5% to 10% in term infants and up to 15% in preterm infants. At lower gestational ages, ECF accounts for a greater proportion of birth weight (
Fig. 23.1). Therefore, very low birth weight (VLBW) infants must lose a greater percentage of birth weight to maintain ECF proportions equivalent to those of term infants. Larger weight loss is possibly beneficial to the preterm infant, as administration of excessive fluid and sodium (Na) may increase risk of chronic lung disease (CLD) and patent ductus arteriosus (PDA).
Sources of water loss
Renal losses. Renal function matures with increasing gestational age (GA). Immature Na and water homeostasis is common in the preterm infant. Contributing factors leading to varying urinary water and electrolyte losses include the following:
Decreased glomerular filtration rate (GFR)
Reduced proximal and distal tubule Na reabsorption
Decreased capacity to concentrate or dilute urine
Decreased bicarbonate, potassium (K), and hydrogen ion secretion
Extra renal losses. In VLBW infants, IWL can exceed 150 mL/kg/day, owing to increased environmental and body temperatures, skin breakdown, radiant warmers, phototherapy, and extreme prematurity (see
Table 23.1). Respiratory water loss increases with decreasing GA and with increasing respiratory rate; in intubated infants, inadequate humidification of the inspired gas may lead to increased IWL. Other fluid losses that should be replaced if amount is deemed significant include stool (diarrhea or ostomy drainage), cerebrospinal fluid (from ventriculotomy or serial lumbar punctures), and nasogastric tube or thoracostomy tube drainage.
Incubators for newborn infants are being designed to improve maintenance of warmth and humidity and may lead to decreased IWL (e.g., the Giraffe isolette).
II. ASSESSMENT OF FLUID AND ELECTROLYTE STATUS
History
Maternal. The newborn’s fluid and electrolyte status partially reflects maternal hydration status and drug administration. Excessive use of oxytocin, diuretics, or hyponatremic intravenous (IV) fluid can lead to maternal and fetal hyponatremia. Antenatal steroids may increase skin maturation, subsequently decreasing IWL and the risk of hyperkalemia.
Fetal/perinatal. The presence of oligohydramnios may be associated with congenital renal dysfunction, including renal agenesis, polycystic kidney disease, or posterior urethral valves. Severe in utero hypoxemia or birth asphyxia may lead to acute tubular necrosis.
Physical examination
Change in body weight. Acute changes in an infant’s weight generally reflect a change in TBW. The compartment affected will depend on the gestational age and clinical course of the infant. For example, long-term use of paralytic agents and peritonitis may lead to increased interstitial fluid volume and body weight but decreased intravascular volume. Therefore, weight should be measured at least daily.
Skin and mucosal manifestations. Altered skin turgor, sunken anterior fontanelle, and dry mucous membranes are not sensitive indicators of fluid or electrolyte balance.
Cardiovascular. Tachycardia can result from ECF excess (e.g., heart failure) or hypovolemia. Capillary refill time can be delayed with reduced cardiac output or peripheral vasoconstriction, and hepatomegaly can occur with increased ECF volume. Blood pressure changes occur late in the sequence of responses to reduced cardiac output.
Laboratory studies
Serum electrolytes and plasma osmolarity reflect the composition and tonicity of the ECF. Frequent monitoring, every 4 to 6 hours, should be done in the extremely low birth weight (ELBW) infants during the first few days of life owing to high IWL.
Fluid balance with input and output measurements should be monitored. Normal urine output is 1 to 3 mL/kg/hour. With ECF depletion (dehydration), urine output may fall to <1 mL/kg/hour. However, in neonates with immature renal function, urine output may not decrease despite ECF volume depletion.
Urine electrolytes and specific gravity (SG) can reflect renal capacity to concentrate or dilute urine and reabsorb or excrete Na. Increases in SG can occur when the infant is receiving decreased fluids, has decreased urine output, or is spilling glucose. Neither urine electrolytes nor SG is very helpful when infant is on diuretics.
Fractional excretion of Na (FENa) reflects the balance between glomerular filtration and tubular reabsorption of Na.
FENa = (urine Na × plasma creatinine)/(plasma Na × urine creatinine) × 100
Level of <1% indicates prerenal factors reducing renal blood flow.
Level of 2.5% occurs with acute renal failure (ARF).
Level of >2.5% is frequently seen in infants of <32 weeks’ gestation.
Blood urea nitrogen (BUN) and serum creatinine (Cr) values provide indirect information about ECF volume and GFR. Values in the early postnatal period reflect placental clearance.
Arterial pH, carbon dioxide tension (Pco2), and Na bicarbonate determinations can provide indirect evidence of intravascular volume depletion because poor tissue perfusion leads to high anion gap metabolic acidosis (lactic acidosis).
III. MANAGEMENT OF FLUIDS AND ELECTROLYTES.
The goal of early management is to allow initial ECF loss over the first 5 to 6 days as reflected by weight loss, while maintaining normal tonicity and intravascular volume as reflected by blood pressure, heart rate, urine output, serum electrolyte levels, and pH. Subsequent fluid management should maintain water and electrolyte balance including requirements for body growth.
The term infant. Body weight decreases by 3% to 5% over the first 5 to 6 days. Subsequently, fluids should be adjusted so that changes in body weight are consistent with caloric intake. Clinical status should be monitored for maldistribution of water (e.g., edema). Na supplementation is not usually required in the first 24 hours unless ECF expansion is necessary. Small-for-gestational-age term infants may require early Na supplementation to maintain adequate ECF volume.
The premature infant. Allow a 5% to 15% weight loss over the first 5 to 6 days.
Table 23.2 summarizes initial fluid therapy. Then, adjust fluids to maintain stable weight until an anabolic state is achieved and growth occurs. Frequently assess response to fluid and electrolyte therapy during the first 2 days of life.
Physical examination, urine output, SG, and serum electrolyte determinations may be required initially as frequent as every 6 to 8 hours in infants < 1,000 g (see
VIII.A.).
Water loss through skin and urine may exceed 200 mL/kg/day, which can represent up to
one-third of TBW. IV Na supplementation is not required for the first 24 hours unless ECF volume loss exceeds 5% of body weight per day (see
Chap. 13). If ECF volume expansion is necessary,
normal saline (NS) is preferred over 5% albumin solutions in order to reduce risk of CLD.
IV. APPROACH TO DISORDERS OF NA AND WATER BALANCE.
Abnormalities can be grouped into disorders of tonicity or ECF volume. The conceptual approach to disorders of tonicity (e.g., hyponatremia) depends on whether the newborn exhibits normal ECF (euvolemia), ECF depletion (dehydration), or ECF excess (edema).
Isonatremic disorders
Dehydration
Predisposing factors frequently involve equivalent losses of Na and water (through thoracostomy, nasogastric, or ventriculostomy drainage) or thirdspace losses that accompany peritonitis, gastroschisis, or omphalocele. Renal Na and water losses in the VLBW infant can lead to hypovolemia despite normal body tonicity.
Diagnosis. Dehydration is usually manifested by weight loss, decreased urine output, and increased urine SG. However, infants of <32 weeks’ gestation may not demonstrate oliguria in response to hypovolemia. Poor skin turgor, tachycardia, hypotension, metabolic acidosis, and increasing BUN may coexist. A low FENa (<1%) is usually seen in infants of >32 weeks’ gestational age (see
II.C.4.).
Therapy. Administer Na and water to first correct deficits and then adjust to equal maintenance needs plus ongoing losses. Acute isonatremic dehydration may require IV infusion of 10 mL/kg of NS if acute weight loss is >10% of body weight with signs of poor cardiac output.
Edema
Predisposing factors include excessive isotonic fluid administration, heart failure, sepsis, and neuromuscular paralysis.
Diagnosis. Clinical signs include periorbital and extremity edema, increased weight, and hepatomegaly.
Therapy includes Na restriction (to decrease total body Na) and water restriction (depending on electrolyte response).
Hyponatremic disorders (see
Table 23.3). Consider
factitious hyponatremia due to hyperlipidemia or
hypoosmolar hyponatremia due to osmotic agents. True hypoosmolar hyponatremia can then be evaluated.