Acquired clitoral enlargement is a rare condition resulting from a variety of etiologies, including tumors and excess androgens. Few cases of nonmalignant schwannoma, a benign tumor of the peripheral nerve sheath, have been reported in the literature as causes of clitoral enlargement in patients without known neurofibromatosis. These painless, slow-growing tumors rarely recur once excised. We present the initial investigation of a patient with a large clitoral schwannoma and subsequent treatment with partial vulvectomy. The workup, including advanced pelvic imaging for diagnosis and surgical planning, as well as removal of the clitoral tumor with preservation of functional tissue and restoration of normal vulvar anatomy despite a large excision, is demonstrated.
Click Video under article title in Contents at ajog.org
Problem
Acquired clitoral enlargement is a rare condition resulting from a variety of etiologies including masses and excess androgens. Few cases of nonmalignant schwannoma have been reported in the literature as causes of clitoral enlargement in patients without known neurofibromatosis.
Schwannomas are tumors of the peripheral nerve sheath that rarely affect the vulva. These tumors can present as slow-growing, painless masses. Surgical excision of clitoral masses can be both diagnostic and therapeutic; however, this can also be difficult when attempting to preserve functional tissue and restore normal vulvar anatomy.
Our solution
We present an individualized plan for surgical management of a complicated clitoral mass in a 38 year old, gravida 1, para 1 with a mass that had slowly increased in size over 28 years. Verbal and written consent was obtained from the patient. She denied any vulvar pain but did have irritation that could be relieved with change of positions. She was sexually active and orgasmic with clitoral stimulation.
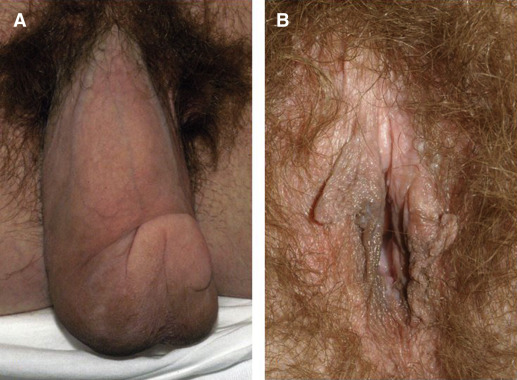
On examination, the clitoris measured 15 cm × 6 cm × 4 cm and was nontender. No other signs of virilization were noted ( Figure 1 A ). An endocrine examination, including follicle-stimulating hormone, luteinizing hormone, prolactin, thyrotropin, free triiodothyronine and thyroxine, dehydroepiandrosterone sulfate, free and total testosterone, and 17-hydroxyprogesterone, was negative for any abnormalities. Given this negative work-up, endocrinology was not consulted.
Advanced pelvic imaging using magnetic resonance imaging was performed using a Philips Ingenia system (Philips, Andover MD). Coronal images of the pelvis were obtained using T2 turbo spin echo sequences (repeat time [TR], 3571; echo time [TE], 100 milliseconds; slice thickness, 5 mm; gap, 0; and number sequence averages [NSA], 1). Axial images of the pelvis were obtained using T2 turbo spin echo sequences (TR, 8460; TE, 80 milliseconds; slice thickness, 4 mm; gap, 0; NSA, 2). Sagittal images of the pelvis were obtained using T1 postcontrast (MultiHance; Bracco, Monroe, NJ) fast field echo; TR, 3.58; TE, 1.70 milliseconds; slice thickness, 1.80 mm; gap, 0; NSA, 4).
This imaging helped to identify clear margins to the clitoral mass and showed that it did not extend into any other pelvic structures. With this information, we were able to plan for surgical excision of the mass. We planned to send a frozen section of the tumor during surgery. The case was discussed with physicians in gynecological oncology, and they were available for intraoperative consultation, if necessary. Given our center’s experience with vulvar surgery, a consultation with plastic surgery was not deemed necessary.
This video demonstrates the surgical treatment via partial vulvectomy and reconstruction to a normal vulvar anatomy with preservation of clitoral tissue ( Video ). Prior to incision, a Foley catheter was placed to delineate the urethra, given its close proximity to the posterior surface of the tumor. The mass extended into and distorted the prepuce and labia minora, which were fused along the posterior surface of the mass. The incision was made for reconstruction of the labia minora with a tension-free closure. The mass was sharply dissected to the stalk identified on magnetic resonance imaging, leaving functional clitoral tissue behind. After cross-clamping and suture ligating the pedunculated stalk, the tumor was sharply excised.
The labia minora were reconstructed with a series of interrupted and vertical mattress sutures. To avoid a dog-ear formation at the lateral corners of the incision, a hockey stick rotational flap was created bilaterally. The remainder of each labium majus was closed using vertical mattress sutures.
The frozen section of the tissue removed in the operating room was benign. The final pathology was a benign plexiform schwannoma, with confirmatory S100 staining. Her recovery was uncomplicated. Four months after surgery, there is no evidence of tumor recurrence, and she has reported normal sexual function with the ability to reach orgasm during clitoral stimulation ( Figure 1 B).
Supplementary data
Plexiform schwannoma: an unusual clitoral mass
Sammarco. Schwannoma of the clitoris. Am J Obstet Gynecol 2016 .
The authors report no conflict of interest.
Cite this article as: Sammarco AG, Abualnadi NM, Andraska EA, et al. Plexiform schwannoma: an unusual clitoral mass. Am J Obstet Gynecol 2017;216:319.e1-2 .
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


