Fig. 35.1
A clinical photograph showing fistula-in-ano in an infant. Note the discharging opening near the anus in (a) and a perianal abscess in (b)
It is considered generally that fistulae-in-ano are a consequence of an underlying perianal infection.
Up to 85 % of children with perianal abscess may progress to form a fistula (Fig. 35.1b).
Perianal abscesses and fistulae-in-ano in neonates are different conditions than those found in older children and adults. They have certain characteristics including:
Much more common in males.
Occur in the majority in infants younger than 1 year of age.
Can be bilateral or have multiple tracts (Fig. 35.2).
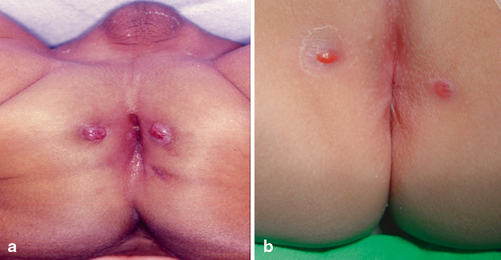
Fig. 35.2
a and b A clinical photograph showing bilateral fistula-in-ano in an infant
The majority are of low type and complex fistulae are rare.
Low incidence of recurrence.
Older children presenting with perianal abscesses or fistulas tend to have a higher incidence of underlying conditions such as inflammatory bowel disease, tuberculosis, or leukemia.
Classification
Congenital type.
Acquired type. This is secondary to:
A perianal abscess
Tuberculosis
Inflammatory bowel disease (Crohn’s disease and ulcerative colitis)
Immunosuppression and leukemia
In the congenital form, the fistulous tract may appear spontaneously or present initially as a perianal abscess .
In the congenital form, the fistulous tract is usually lined with stratified squamous epithelium, columnar epithelium, or both.
The acquired form manifests with repeated perianal abscesses and has an inflamed fibrous tract lined by granulation tissue with no epithelial lining upon microscopic examination.
Perianal abscesses in male infants usually grow enteric organisms (E. coli, coliforms, pseudomonas, proteus, etc.) while female infants with perianal abscess usually grow Staphylococcus aureus. This is of importance as the majority of male infants who present with perianal abscess will subsequently develop fistula-in-ano which is not the case in female infants.
Etiology
The exact etiology of fistula-in-ano is not known and several factors have been suggested.
Fistula-in-ano in an otherwise healthy neonate is suspected to originate as anal cryptitis, which progresses to form a perianal abscess .
Hormonal imbalance:
It has been postulated that androgen excess or androgen–estrogen imbalance may cause the formation of abnormal crypts of Morgagni with a predisposition to cryptitis and abscess formation.
Androgen excess: This may stimulate the sebaceous glands, resulting in secondary infection with perianal abscess formation and fistulae.
Abnormal crypts of Morgagni:
Although the etiology of abnormal crypt formation remains unknown, it has been shown that the crypts of infants with fistulas tend to be deeper (3–10 mm) than crypts seen in normal infants (1–2 mm).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


