Pelvis Mass
Eva Ilse Rubio, MD
DIFFERENTIAL DIAGNOSIS
Common
Ovarian Lesion, Nonneoplastic
Simple Cyst
Parovarian Cyst
Hemorrhagic Cyst
Ovarian Lesion, Neoplastic
Germ Cell Tumors
Stromal Cell Tumors
Epithelial Cell Tumors
Ovarian Torsion
Duplication Cyst, GI Tract
Less Common
Genitourinary Anomalies
Obstructed Urinary Bladder
Horseshoe Kidney
Cloaca
Hydrometrocolpos/Hematometrocolpos
Lymphoma (Burkitt)
Sacrococcygeal Teratoma
Anterior Sacral Meningocele
Neuroblastoma
Desmoid
Ewing Sarcoma
Rhabdomyosarcoma, Genitourinary
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Gender and age of patient
Helpful Clues for Common Diagnoses
Ovarian Lesion, Nonneoplastic
Simple Cyst
Anechoic, larger than 3-5 cm
If large, may cause torsion; occasionally large enough to extend into abdomen
Parovarian Cyst
Wolffian duct remnant; anechoic
Appearance/size will not change with time
Hemorrhagic Cyst
Appearance depends on chronicity
May be echogenic/solid, lacy/septated, or mixed with fluid-debris levels
Ovarian Lesion, Neoplastic
Germ Cell Tumors
Various types: Teratoma, dysgerminoma, yolk sac tumor, embryonal cell carcinoma, choriocarcinoma
Most common teratoma features are
Mixed cystic, solid, calcified elements
Fat within lesion well seen on CT
Identifying teeth “clenches” diagnosis
May be bilateral
“Tip of iceberg” sign: Posterior acoustic shadows of teeth/bone/calcifications obscure full extent of mass
Stromal Cell Tumors
Granulosa cell tumor: Often solid; may cause sexual precocity
Leydig cell tumors: Cystic, solid, or mixed; often cause virilization
Epithelial Cell Tumors
e.g., cystadenoma, cystadenocarcinoma
Predominantly cystic appearance
Uncommon in children
Ovarian Torsion
Marked asymmetry in ovarian volumes
Appearance varies with chronicity
Hypoechoic or heterogeneous
Peripheral follicles often seen
Presence of blood flow may reflect intermittent torsion or multiple vessels serving ovary
Underlying cyst or mass is common
Duplication Cyst, GI Tract
Often round or tubular; may be multiple
Hypoechoic on US, low attenuation on CT
On US may see bowel wall layers (echogenic mucosa, serosa, intervening hypoechoic muscularis)
Helpful Clues for Less Common Diagnoses
Genitourinary Anomalies
Obstructed Urinary Bladder
Must search for structural anomalies, i.e., posterior urethral valves, cloaca, spinal cord anomaly, obstructing mass
Horseshoe Kidney
May be partially obstructed or multicystic
Increased risk of infections, Wilms tumor, or injury (superficial location)
Cloaca
Large fluid-filled structure(s) often seen
Complex anatomic abnormalities associated with anorectal malformations, vaginal/uterine anomalies
Search for coexisting upper urinary tract anomalies or obstructive hydronephrosis
Hydrometrocolpos/Hematometrocolpos
Lymphoma (Burkitt)
Commonly involves abdominal/pelvic organs, especially distal bowel
Clinically causes obstruction or intussusception
Suggestive imaging findings
US: Hypoechoic, mildly heterogeneous
CT: Homogeneous, wall thickening, adenopathy
MR: Homogeneous, intermediate/bright signal
Sacrococcygeal Teratoma
Heterogeneous, mixed cystic/solid mass
Calcifications common but not universal
Prognosis depends on prompt diagnosis; higher risk of malignancy after 2 months
Type 1 is extrapelvic
Type 2 is predominantly extrapelvic, small intrapelvic component
Type 3 is predominantly intrapelvic, small extrapelvic component
Type 4 is entirely intrapelvic, delayed diagnosis is therefore common
Anterior Sacral Meningocele
Usually purely cystic in appearance
Few associated with Currarino triad
Other considerations: Neurofibromatosis, Marfan syndrome
Neuroblastoma
Arises from neural crest cells in sympathetic chain ganglia or adrenal medulla
Poorly marginated, encases vessels
Typical CT/US/MR findings
Heterogeneous soft tissue mass with calcifications, necrosis, hemorrhage
Metastases typically to liver, skin (younger ages), and bones (older children)
Desmoid
Benign tumor with well-marginated or infiltrating margins
CT and MR imaging characteristics depend upon histologic features, relative amounts of collagen, spindle cells
Ewing Sarcoma
Pelvic origin not uncommon
Soft tissues: Large heterogeneous mass is commonly seen
Bone: May be lytic, sclerotic, or mixed, with periosteal reaction
Rhabdomyosarcoma, Genitourinary
May arise from any pelvic structure: Bladder, vagina, uterus, or prostate
Polypoid appearance is typical but not universal
Hydronephrosis is common finding
Image Gallery
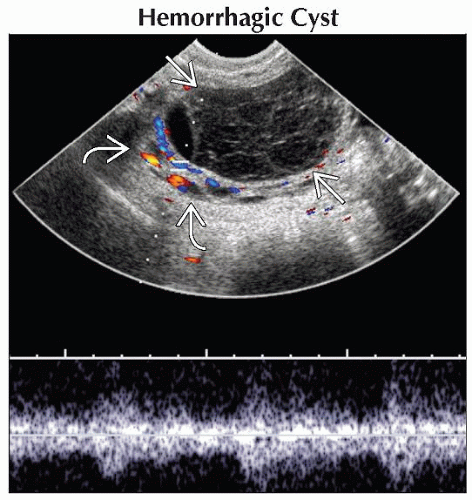 Longitudinal ultrasound shows a circumscribed, hypoechoic, septated, ovoid pelvic mass  . There is a crescent of normal ovarian tissue, seen with normal Doppler signal, stretched along its edge . There is a crescent of normal ovarian tissue, seen with normal Doppler signal, stretched along its edge  . . |
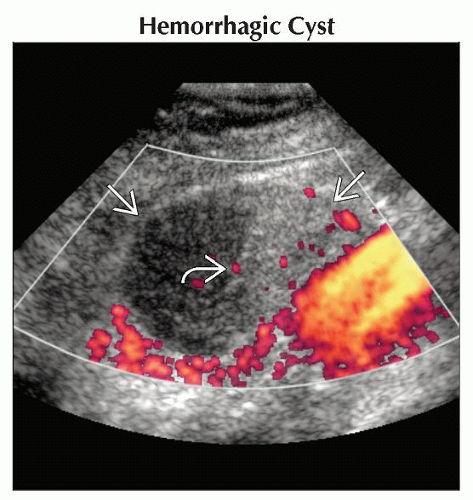 Longitudinal ultrasound shows a well-defined oval lesion  with no blood flow (gain is turned up high). Note the fluid-debris level with no blood flow (gain is turned up high). Note the fluid-debris level  . This hemorrhagic cyst involuted over time. . This hemorrhagic cyst involuted over time. |
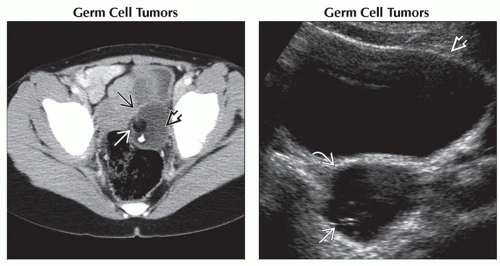 (Left) Axial CECT shows an ovoid pelvic lesion
 in the generally expected region of the left ovary. Note the classic components: Fluid-containing cyst in the generally expected region of the left ovary. Note the classic components: Fluid-containing cyst  , low-attenuation fat , low-attenuation fat  , and a tooth. (Right) Transverse ultrasound shows a round lesion , and a tooth. (Right) Transverse ultrasound shows a round lesion  posterior to the bladder posterior to the bladder  . The lesion is predominantly cystic with an ill-defined, linear, echogenic area that represents fat or hair . The lesion is predominantly cystic with an ill-defined, linear, echogenic area that represents fat or hair  . .Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|