Elbow Effusion
Christopher G. Anton, MD
DIFFERENTIAL DIAGNOSIS
Common
Supracondylar Fracture
Lateral Condylar Fracture
Medial Epicondyle Avulsion
Trauma without Fracture
Radial Neck Fracture
Other Less Common Fractures
Less Common
Osteochondritis Dissecans
Juvenile Idiopathic Arthritis (JIA)
Septic Arthritis
Panner Disease
Rare but Important
Tumor
Hemophilia
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Anatomy
Elbow ossification center appearance (CRITOE)
Capitellum, radial head, medial (internal) epicondyle, trochlea, olecranon, lateral (external) epicondyle
Trauma
Anterior humeral line
Lateral view: Line should pass through middle 1/3 of capitellum
When anterior humeral line is abnormal, may indicate minimally displaced supracondylar fracture (fx)
Coronoid line
Line along volar border of coronoid process should barely contact volar portion of lateral condyle on lateral view
Radiocapitellar line
Line drawn from center of radial shaft that normally extends through capitellar ossification center
Not necessarily passing through middle 1/3 of capitellum
When abnormal, radial head dislocation is likely
Teardrop
On lateral view, dense anterior line reflects posterior margin of coronoid fossa
Posterior dense line reflects anterior margin of olecranon fossa
Fat pad signs
Anterior fat pad: Nondisplaced and visualized in normal elbows
If elevated (“sail” sign), consider joint effusion; if trauma history, must exclude occult fx
Supinator fat pad: Anterior aspect of supinator muscle along proximal radius; if displaced, consider radial neck fx
Posterior fat pad sign more sensitive to underlying occult elbow fx
Joint capsule must be intact to detect fat pad displacement
Helpful Clues for Common Diagnoses
Supracondylar Fracture
˜ 50-70% of elbow fxs in children
Most commonly extension type injury
Age: 3-10 years old
Cubitus varus (calculated by Baumann angle) most common complication
Vascular injury: Most serious complication
Displaced fx: 10-15% injury rate for anterior interosseous branch of median nerve injury
Lateral Condylar Fracture
˜ 20% of elbow fxs in children
Age: typically 4-10 years old
Fx line parallels metaphyseal margin of lateral physis
Oblique views are often helpful in detection and assessing amount of displacement
≥ 2 mm of displacement may require open surgical reduction and pinning
Nondisplaced fxs: Posterior splint and lateral gutter
Medial Epicondyle Avulsion
Displacement > 5 mm, surgical reduction
Valgus stress with avulsion from flexor-pronator muscle group
50% associated with elbow dislocations
Should see medial epicondyle on AP radiograph if trochlea is identified
May become displaced and trapped into elbow joint; simulates trochlear ossification center
Unreliable fat pad sign; tends to be extracapsular in location in children > 2 years old
Trauma without Fracture
If elbow effusion initially found without detection of fx, > 80% likelihood of seeing fx on follow-up radiographs
Radial Neck Fracture
Most cases are Salter-Harris type 2 fxs (90%); average age of 10 years
Other Less Common Fractures
Transphyseal fracture
< 2 years old, > 50% result of nonaccidental trauma
May be mistaken for elbow dislocation; in true dislocation, radiocapitellar (RC) line is disrupted
Capitellum still aligns with radial head
Olecranon (normal ossification center can be mistaken for fx), intercondylar, medial condylar, radial head dislocation
Helpful Clues for Less Common Diagnoses
Osteochondritis Dissecans
a.k.a. osteochondral lesion
Medial femoral condyle is most common site
Elbow: Most commonly anterolateral aspect of capitellum
Typically adolescent boys (> 13 years old)
Related to repetitive valgus stress and impaction with radial head
Juvenile Idiopathic Arthritis (JIA)
Begins < 16 years old, symptoms > 6 weeks
Systemic, pauciarticular, polyarticular
Pannus, synovial proliferation, joint effusion, erosions
Septic Arthritis
Infection via bloodstream but may become infected due to injection, surgery, or injury
Staphylococcus aureus most common pathogen
Most common symptoms: Fever, arthralgia, and joint swelling
< 1/2 have arthritis and osteomyelitis
Panner Disease
Osteochondrosis of capitellum
Capitellar ossification center irregular mineralization, similar changes to Legg-Calvé-Perthes disease
Most commonly: Boys 5-12 years old, dominant arm
Distinguish from osteochondritis dissecans (patients > 13 years old)
± effusion
Helpful Clues for Rare Diagnoses
Tumor
Chondroblastoma, giant cell tumor, Langerhans cell histiocytosis, etc.
Hemophilia
Bleeding disorder; knee, elbow, ankle, hip, and shoulder most commonly involved joints
Diagnosis usually known prior to imaging
Joint effusion may appear radiodense on conventional radiographs
MR: Subchondral erosion, synovial proliferation, joint effusion, hemosiderin deposition
Image Gallery
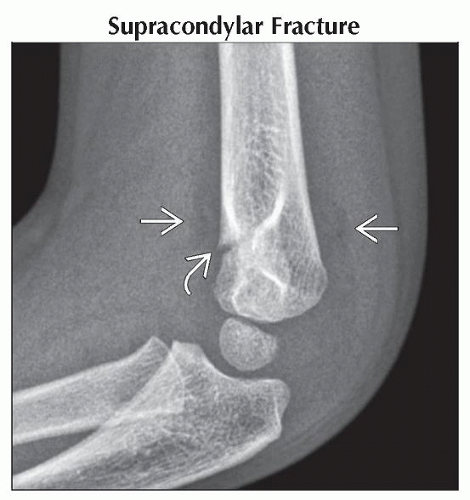 Lateral radiograph shows displacement of the anterior (“sail” sign) and posterior fat pads
 due to hemarthrosis. Note the fracture line due to hemarthrosis. Note the fracture line  through the volar cortex of the distal humerus. through the volar cortex of the distal humerus.Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|