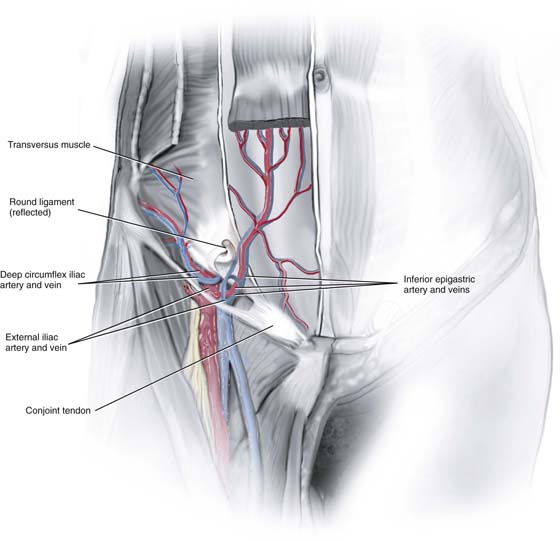
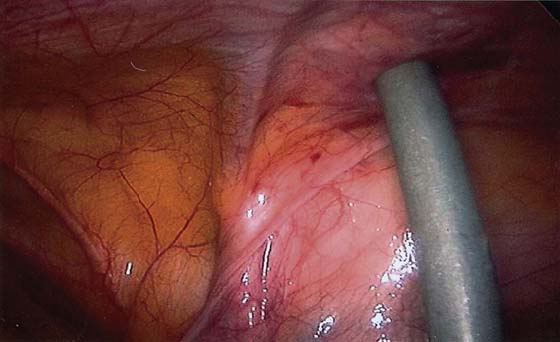
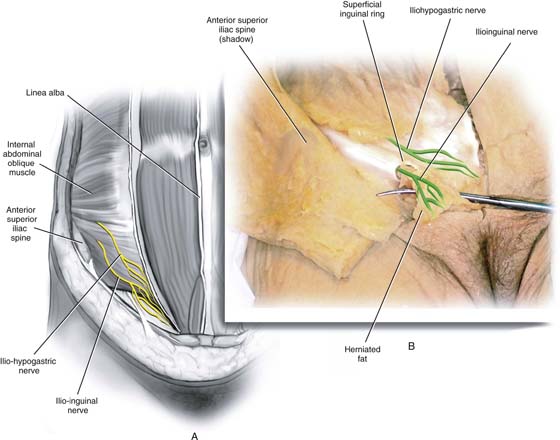
CHAPTER 113 Tommaso Falcone The anatomic view of the pelvis through a laparoscope can be somewhat disorienting to the pelvic surgeon. However, the same basic principle of understanding the relationship between important structures can be a guide. This chapter is an overview of some of the most commonly seen anatomic structures that should be visualized during most pelvic laparoscopic procedures. An understanding of the anterior abdominal wall anatomy is critical for proper placement of the trocars required for laparoscopy. The anatomy of the inferior epigastric vessels and their relationship to the placement of accessory ports are covered in the chapter on trocar placement. The external iliac artery has two branches: the inferior epigastric artery and the deep circumflex iliac artery. The inferior epigastric artery branches from the external iliac artery at the level of the inguinal ligament. It is seen medial to the insertion of the round ligament at the deep inguinal ring and then courses medially anterior to the peritoneum toward the rectus muscle. It can easily be seen because of the lack of fascia at this level (Fig. 113–1). It forms a fold of peritoneum called the lateral umbilical fold. Two veins usually accompany the inferior epigastric artery (Fig. 113–2). It then ascends behind the muscle and anterior to the posterior rectus sheath to anastomose with the superior epigastric vessel. Two important nerves can be injured by the introduction of the trocar or closure of the port sites: the iliohypogastric and ilioinguinal nerves (Fig. 113–3). The iliohypogastric nerve originates from L1 and traverses through the abdominal muscles; its anterior cutaneous branch pierces the internal oblique muscle 2 cm medial to the anterior superior iliac spine (ASIS). It then travels between the internal and external oblique aponeurosis until it pierces the latter aponeurosis about 3 cm above the superficial inguinal ring. The ilioinguinal nerve also originates from L1 and traverses the internal oblique aponeurosis approximately 2 cm medial to the level of the ASIS. It travels between the external oblique and internal oblique aponeurosis and enters the inguinal canal to emerge from the superficial inguinal ring. These nerves are sensory to the ipsilateral mons pubis and labia majora; injury to them can cause paresthesia. Entrapment can cause pain over the nerve distribution. Insertion of accessory trocars above the ASIS usually avoids this injury. FIGURE 113–1 The trocar is lateral to the right inferior epigastric vessels seen within the peritoneal fold. FIGURE 113–2 The right round ligament has been transected, and the inferior epigastric vessels (one artery and two veins) are seen medial to it. FIGURE 113–3 A. The external oblique aponeurosis has been removed, and the two nerves are seen on the internal oblique muscle arising 2 cm medial to the right anterior superior iliac spine. B. The terminal branches of the two nerves are seen. The ilioinguinal nerve exits the superficial inguinal ring. The aortic bifurcation occurs approximately at the level of L4. In nonobese patients, this is found at the level of the umbilicus. With increasing weight, the umbilicus is located more caudad to the bifurcation. Typically, a trocar or pneumoperitoneum needle is angled at 45° to avoid the aorta. However, the major vessel that is seen below the bifurcation of the aorta is the left common iliac vein, which can be injured when the primary umbilical instrument is introduced (Figs. 113–4
Pelvic Anatomy From the Laparoscopic View
 Mark D. Walters
Mark D. Walters
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


