Fig. 61.1
a and b Clinical photographs showing large abdominal mass due to mesenchymal hamartoma
Alpha-fetoprotein level may be elevated.
Abdominal X-ray may show calcification (Fig. 61.2).
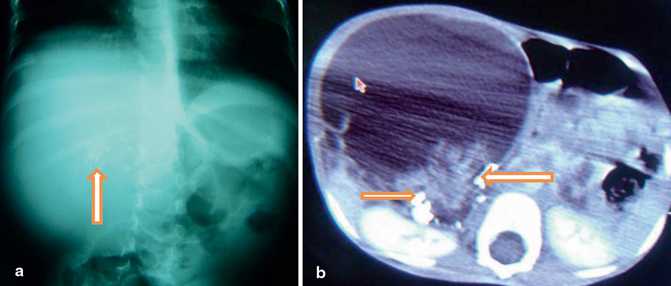
Fig. 61.2
Abdominal X-ray showing a soft tissue density mass with calcification (a) and abdominal CT scan showing a large liver tumor with calcification (b)
Abdominal CT scan and MRI reveal a well-circumscribed, multilocular cystic mass with solid septae and stroma (Fig. 61.3).
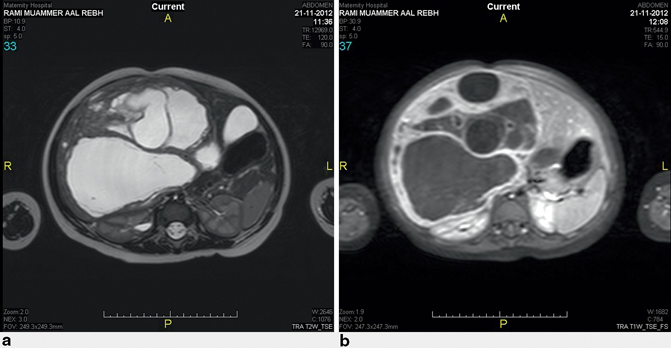
Fig. 61.3
a and b Abdominal MRI showing multicystic liver tumor
Enucleation and marsupialization of the mass are treatment options.
Complete surgical excision with a rim of normal liver tissue is the treatment of choice (Figs. 61.4 and 61.5).
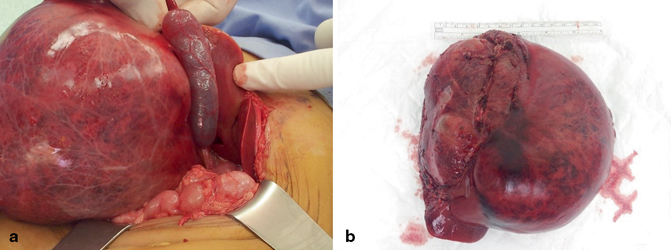
Fig. 61.4
Intraoperative photograph showing a large liver tumor arising from the right lobe of the liver (a) and a clinical photograph showing a large mesenchymal hamartoma after total excision (b)
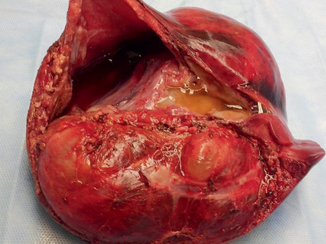
Fig. 61.5
A clinical photograph showing a large liver mesenchymal hamartoma. Note the multiple cysts
There are reports of sarcoma and hepatoblastoma arising from mesenchymal hamartoma.
Mesenchymal hamartomas have a tendency to recur, which makes complete excision the treatment of choice.
Focal Nodular Hyperplasia and Hepatic Adenomas
Focal nodular hyperplasia and hepatic adenomas are rarely seen in children.
Both of these benign tumors have an association with high estrogen and frequently occur in adolescent girls.
Hepatic adenomas are associated with oral contraceptive use.
Usually, they are asymptomatic or cause nonspecific symptoms including abdominal pain and mass (Fig. 61.6).
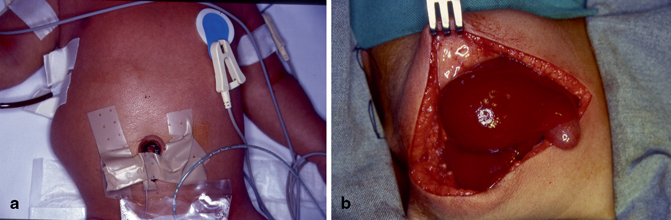
Fig. 61.6
Clinical (a) and intraoperative (b) photographs showing focal nodular hyperplasia of the liver which was resected
A characteristic central scar on CT scan is pathognomonic for focal nodular hyperplasia.
A three-phase CT scan is the investigation of choice to make the diagnosis of focal nodular hyperplasia.
A technetium sulfur colloid scan is used to differentiate focal nodular hyperplasia from adenomas. This reveals uniform uptake by focal nodular hyperplasia.
Open liver biopsy may be required for definitive diagnosis.
Focal nodular hyperplasia has no malignant potential and is often asymptomatic.
Many surgeons advocate elective resection of focal nodular hyperplasia to prevent spontaneous rupture and hemorrhage (Fig. 61.6).
Other surgeons advocate follow-up of these patients with serial ultrasounds.
If the lesions are symptomatic or rapidly enlarging, complete surgical resection, embolization, or hepatic artery ligation may be used for treatment.
Hepatic adenomas are treated with complete surgical excision because these lesions have a small risk for:
Spontaneous rupture
Hemorrhage
Malignant transformation to hepatocellular carcinoma
Hepatocellular Carcinoma
Hepatocellular carcinoma is rare in children and accounts for 23 % of pediatric hepatic malignancies .
Hepatocellular carcinoma typically presents in two incidence peaks :
The first is at age 0–4 years
The second is at age 10–14 years
Predisposing conditions include:
Hepatic fibrosis and cirrhosis secondary to:
◦ Metabolic liver disease
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


