Osteosarcoma
Richard Gorlick and Paul A. Meyers
Osteosarcoma is the most common malignant primary bone tumor in children and adolescents. 
The diagnosis of osteosarcoma can be made based on histologic examination of pathologic material, staging can be performed with imaging procedures, and multimodality therapy including chemotherapy and surgery successfully treat the majority of patients. Despite all of these advances, osteosarcoma remains enigmatic. The biology of the tumor is incompletely understood, and recent trials modifying therapy have failed to produce further advances. Patients with localized disease have a 5-year survival of at least 70%; patients with metastatic or recurrent disease have a < 20% chance of long-term survival despite aggressive therapies. These figures have changed little in the past 2 decades.3-6
 EPIDEMIOLOGY/ETIOLOGY
EPIDEMIOLOGY/ETIOLOGY 
Osteosarcoma has a bimodal age distribution with the first peak in the second decade of life and the second among older adults. The approximate incidence of osteosarcoma is 4.8 per million children younger than 20 years of age.7 There are approximately 400 new cases per year in those under 20 years of age in the United States.8 Primary bone tumors account for approximately 5% to 10% of all new pediatric cancer diagnoses in the United States, of which osteosarcoma is the most common.7 The male-to-female ratio is approximately 1.3:1 in this age range. 
The peak age of incidence coincides with a period of rapid bone growth in young people, which suggests a correlation between bone growth and the evolution of osteosarcoma.8,9
 CLINICAL PRESENTATION
CLINICAL PRESENTATION
The most common features in the clinical presentation of osteosarcoma are pain and swelling in the involved region, with or without an associated soft tissue mass. Symptoms are usually present for several months before the diagnosis is made. The median time from onset of symptoms to diagnosis is 4 months.242-246 Occasionally, patients present more dramatically with a pathologic fracture. The most common primary site is the metaphysis of a long bone, but osteosarcoma can occur in any bone of the body. Approximately half of all osteosarcomas originate in the region around the knee.40,41 The most common sites of disease are the distal femur, the proximal tibia, and the proximal humerus. The anatomic distribution of osteosarcoma is shown in Figure 453-1.7 Approximately 20% of patients present with radiographically detectable metastatic disease. Eighty percent of patients present with localized disease, but the vast majority of this group are known to have subclinical, microscopic metastases.8 The most frequent site of metastases is the lung. The vast majority of patients at presentation do not have systemic symptoms such as fever or weight loss even with overt meta-static disease. Death from osteosarcoma is almost always the result of progressive pulmonary metastasis.8 Bone lesions, although extremely painful, are usually not life threatening.3-6,8,240
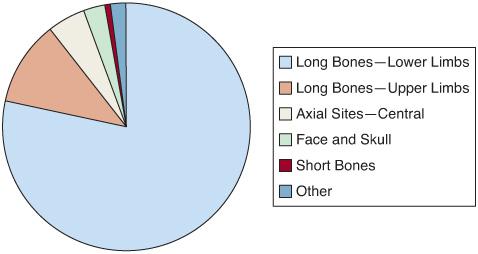
FIGURE 453-1. Anatomic site distribution of osteosarcoma in individuals less than 20 years of age.7
 EVALUATION
EVALUATION
The evaluation of suspected osteosarcoma begins with history, physical examination, laboratory evaluations, and plain radiographs. History may be significant only for pain. Physical examination is typically remarkable only for a soft tissue mass, not always present, at the primary site.3-6,8,240,241 Laboratory evaluation is seldom revealing. Elevation of the serum alkaline phosphatase and lactate dehydrogenase is observed in a large proportion of patients but is not sensitive or specific.8 In a patient with a suspected bone tumor, obtaining a plain radiograph of the site is critical for making an appropriate diagnosis.3-6,8,240,241
In a patient with a suspected bone tumor, obtaining a plain radiograph of the site is critical for making an appropriate diagnosis.3-6,8,240,241
The diagnosis of osteosarcoma is typically suspected from its radiographic appearance. Osteosarcoma can present as a lytic, a sclerotic, or a mixed lytic-sclerotic lesion. Ossification in the soft tissue suggestive of bone spicule formation in a “sunburst”’ pattern is classic for osteosarcoma but is not a sensitive or specific feature.40,41 Cortical destruction with periosteal new bone formation can lead to the appearance of a Codman’s triangle. In addition to the lesion’s appearance, features such as location in the metaphysis and the bone involved as well as the patient’s age help to distinguish osteosarcoma from other clinical entities.40,41 Appearance of the tumor on plain radiographs can be highly suggestive of the diagnosis. A typical radiograph of a patient with an osteosarcoma in the femur is shown in Figure 453-2. Despite the utility of plain radiographs, computerized tomography (CT) and magnetic resonance imaging (MRI) both offer improved resolution and better delineation of tumor extension and are routinely performed with suspected osteosarcoma.247-249
It is mandatory to obtain a biopsy for pathological confirmation of the diagnosis. 
 STAGING
STAGING
Prior to initiation of therapy, accurate staging is necessary to determine the extent of disease which has prognostic significance.257 Routine posteroanterior and lateral radiographs of the chest allow detection of metastases in the majority of cases. CT of the chest is more sensitive in detecting pulmonary metastases and has become the imaging procedure of choice.258

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


