Fig. 37.1
Clinical photograph showing omphalocele. Note the location of the omphalocele in the center of the umbilical cord
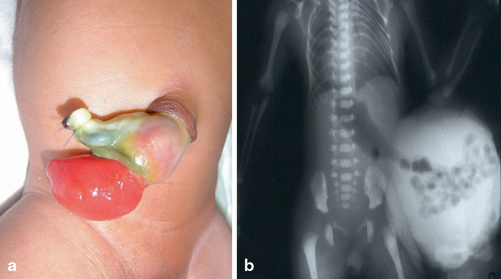
Fig. 37.2
Abdominal x-ray showing omphalocele and a clinical photograph showing ruptured omphalocele
The incidence of omphalocele is variable but generally occurs in 2.5/10,000 births. Small omphaloceles on the other hand occur with a rate of 1 case in 5000 live births. Large omphaloceles occur with a rate of 1 case in 10,000 live births.
The mean size of omphalocele defect is 2.5–5 cm (4–12 cm).
Omphalocele is classified into two types: minor and major.
Minor omphalocele: There is protrusion of a small portion of the intestine only and the size of the defect is < 5 cm in diameter.
Major omphalocele: There is protrusion of the intestines, liver, and other organs and the diameter of the defect is > 5 cm.
The omphalocele sac is ruptured in 10–20 % of cases. This may occur in utero or during delivery (Fig. 37.2b).
Etiology
The exact etiology of omphalocele is not known.
Various theories have been postulated; these include:
Failure of the bowel to return into the abdomen by 10–12 weeks
Failure of lateral mesodermal body folds to migrate centrally
Persistence of the body stalk beyond 12 weeks’ gestation
A defect in the development of the muscles of the abdominal wall.
Diagnosis
Omphalocele is usually detected antenatally during routine ultrasonographic evaluation.
An omphalocele is diagnosed when an anterior midline abdominal mass is demonstrated on fetal ultrasonic evaluation.
The mass consists of abdominal contents that have herniated through a midline central defect at the base of the umbilical cord insertion. The mass usually has a smooth surface and contains abdominal viscera, usually the liver, intestines, and stomach.
Diagnostic amniocentesis is indicated when an omphalocele is demonstrated on antenatal ultrasound evaluation. This is to detect associated chromosomal abnormalities.
The finding of an omphalocele should prompt a detailed ultrasonographic evaluation to detect associated anomalies.
Fetal echocardiography and karyotyping should also be performed.
Associated Anomalies
Omphaloceles are associated with other anomalies in 70−80 % of the cases.

Fig. 37.3
Clinical photograph showing ruptured omphalocele with ruptured Meckel’s diverticulum
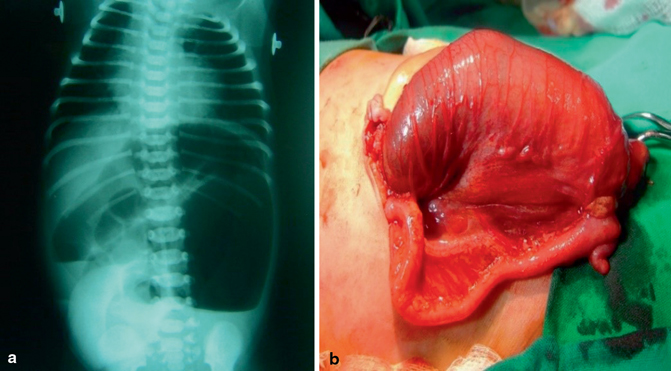
Fig. 37.4
Plain abdominal x-ray showing features of intestinal obstruction in a patient with omphalocele (a) and a clinical photograph showing intestinal atresia in a patient with omphalocele (b)
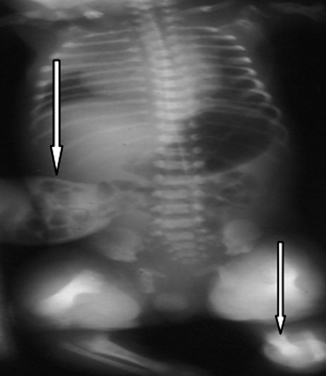
Fig. 37.5
Plain x-ray showing skeletal malformations in a patient with omphalocele
Congenital heart disease (25 %): Most commonly ventricular septal defect, atrial septal defect, and tetralogy of Fallot.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


