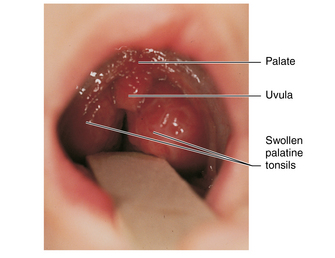
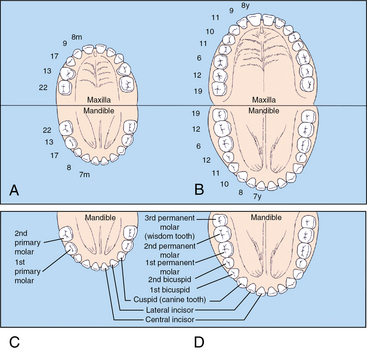
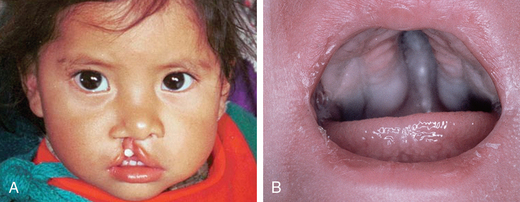
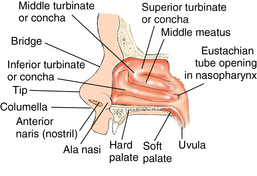
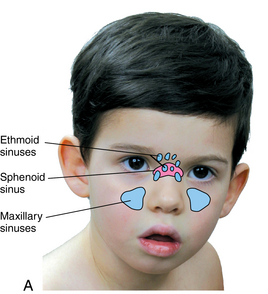
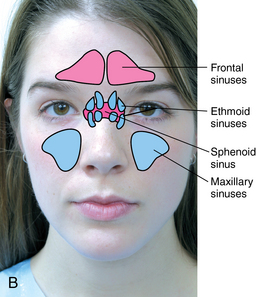
CHAPTER 13 Early development of the nose begins during the fifth week of gestation, with development of muscle, bone, and cartilage complete by the twelfth week of gestation. The palate evolves from fusion of the maxillary prominences during the seventh and eighth weeks of gestation and is completely formed by the twelfth week of gestation during the fusion of the primary and secondary palates. Failure in fusion results in cleft palate. Cleft palate is a relatively common congenital anomaly and occurs in 1 in 700 births1 (Figure 13-1). The incidence varies with race, with Native Americans having a rate of 3.6 in 1000 births, and blacks having the lowest rate of 0.3 in 1000 births.2 It can be an isolated defect, bilateral cleft, associated with cleft lip, or a component of a syndrome.2 The etiology is usually unknown, but genetics is thought to be involved in both syndromic and nonsyndromic clefts. Environmental factors may increase the risk of cleft palate; folic acid deficiency, ingestion of some teratogens such as alcohol and phenytoin (Dilantin), and maternal smoking have also been implicated. A subcutaneous cleft also can occur during this period with incomplete fusion of the palate; it often goes undetected in the newborn and is associated with persistent abnormal speech patterns. Table 13-1 presents the developmental variations to be monitored from infancy to adolescence. Table 13-2 reviews the development of the sinuses from infancy through adolescence. TABLE 13-1 Physiological Variations of the Nose, Mouth, and Throat TABLE 13-2 Data from Schoem SR, Darrow DH: Pediatric otolaryngology, Elk Grove Village, IL, 2012, American Academy of Pediatrics. The nose of the newborn and young infant is generally flattened and malleable (Figure 13-2). In the neonate, the septum is composed of cartilage; ossification occurs during childhood. The nose becomes pyramid-like by adolescence and develops a bony structure. It is divided into four sections: the proximal bony portion, often referred to as the nasal bridge; the mid cartilaginous vault; the tip, columella and nares; and the interior vestibule (Figure 13-3). Nasal breathing is the normal breathing pattern, and infants and young children are prone to increased airway resistance because they have anatomically small airway passages. Nasal congestion in the neonate is a common normal finding, and newborn nurseries often discharge infants with a nasal bulb syringe to enable the gentle removal of secretions from the small narrow nasal passages. In the past, it was thought that newborns are obligatory nasal breathers for the first few months of life. However, research has demonstrated newborns have the ability to switch from nasal to mouth breathing as needed, so they are “preferential” nasal breathers.2 Respiratory compromise or distress occurs rapidly in the young infant when the nasal passages become occluded. The most common reason for occlusion is mucosal congestion or increased secretions, but congenital anatomical deformities, obstructive masses, or traumatic obstruction can occlude the nasal passages. Nasal resistance may result in 50% of the total airway resistance being largely determined by the size of the airway passages. The internal nose, the vestibule, is divided by the bony and cartilaginous nasal septum. The septum is rarely perfectly straight and a significant deviation of the septum resulting from the birth process or trauma must be assessed to determine whether it interferes with nasal breathing. The perpendicular plate of the nasal septum ossifies by 3 years of age. The anterior portion of the vestibule is lined with vascular squamous epithelium that has tiny hair follicles and secretes mucus. The vast majority of nose bleeds, or epistaxis, result from a network of small blood vessels found in the anterior superficial portion of the septal mucosa known as the Kiesselbach plexus. The posterior portion is lined with fragile respiratory epithelium. The lateral walls of the nose are composed of horizontal bony structures known as the superior, middle, and inferior turbinates, which mature throughout childhood and resemble those of the adult by 12 years of age (see Figure 13-3). They are covered with vascular mucous membranes. Furrows between the bony structures provide recesses to filter air and form a nasal passage, or meatus. The posterior ethmoid sinuses drain into the superior meatus, and the paranasal sinuses drain into the middle meatus. Until approximately 6 years of age, the inferior meatus is nonfunctioning except that it drains the nasolacrimal duct. This is why the nose has increased drainage in children, particularly during periods of crying or eye irritation. The space between the posterior portion of the turbinates and the posterior wall of the nasopharynx is called the choana and is of little significance in children unless blocked by a congenital abnormality such as choanal atresia, a bony or membranous blockage of the naris posterior to the nasal turbinates, resulting in blockage of the airway. It occurs in 1 in 10,000 births.3 The nasopharynx forms the superior portion of the pharynx. The eustachian tube opening is located along the lateral walls of the nasopharynx (see Figure 13-3). Adenoidal tissue is found along the superior posterior wall of the oropharynx and is referred to as the pharyngeal tonsils. The inferior border of the nasopharynx is formed by the soft palate. The nasopharynx is surrounded by bone, ensuring patency unless trauma occurs. The paranasal sinuses consist of paired cavities: maxillary, ethmoid, frontal, and sphenoid sinuses. The maxillary and ethmoid sinuses are present at birth but are small, and the sphenoid and frontal sinuses develop during infancy and early childhood. The sinuses become air-filled cavities lined with ciliated epithelium containing goblet cells and submucosal glands that produce seromucinous secretions and immune mediators as they develop and mature within the sinus cavity. The sinuses reach their final form between 12 and 14 years of age2 (Figure 13-4; see Table 13-2). The oral cavity is composed of the lips, cheeks, hard and soft palates, teeth, posterior pharynx, tongue, sensory cells for taste, and the mandible that supports the lower gums and teeth (Figure 13-5). The cheeks form the lateral walls lined with buccal mucosa. Cheeks may be particularly prominent in young children because of the buccal fat pad. The cheeks and lips are innervated by cranial nerves V (trigeminal) and VII (facial). The central nervous system controls the complex mechanisms of the mouth needed for sucking, swallowing, breathing, and vocalization. The hard palate is the anterior two thirds of the palate and separates the nasal and oral cavities. The posterior third of the palate is the soft palate, which is contiguous with the lateral pharyngeal wall. It provides a slightly mobile barrier between the nasopharynx and oropharynx and is essential for normal articulation and speech intonation. The palatine tonsils form the anterior and posterior tonsillar pillars. Tonsillar size is graded on a scale of 1+ to 4+ (Table 13-3 and Figure 13-6). Additional tonsillar tissues surround the posterior pharynx but are not visible on examination. The uvula hangs down from the middle of the soft palate in line with the anterior pillar, or palatoglossus muscle. A bifid uvula, a cleft with two parts, is an anomaly that results from disruption of the palate development and may indicate a submucosal cleft palate. It may also be associated with nasal polyps and is more common in children with cystic fibrosis. TABLE 13-3 FIGURE 13-6 Enlarged tonsils in child. (From Thibodeau G, Patton K: The human body in health and disease, ed 5, St. Louis, 2010, Mosby.) The mandibular central incisors are the first to erupt in the majority of infants, followed by the maxillary central incisors then the upper and lower lateral incisors, first molars, cuspids or canine teeth, and then the second molars. Tooth eruption, movement of the tooth through alveolar bone and gums, normally occurs between 4 and 12 months of age for the first tooth, and takes place when about two thirds of the root for the tooth is developed. The maxillary incisors usually erupt 1 to 2 months after the mandibular incisors. The eruption of the 20 primary teeth should be complete between 24 and 30 months of age (Figure 13-7, A). The timing and sequence of tooth eruption depend on genetic, nutritional, environmental, and systemic factors. Delayed eruption of the primary teeth can occur in premature infants, infants small for gestational age, infants or children with metabolic or chromosomal abnormalities, or children with severe malnutrition. A family pattern of delayed tooth eruption can also occur across generations. FIGURE 13-7 Ages of tooth eruption. A, Primary dentition of maxilla. B, Permanent dentition. C, Primary dentition of mandible. D, Permanent dentition of mandible. (From Zitelli BJ, Davis HW: Atlas of pediatric physical diagnosis, ed 4, St. Louis, 2002, Mosby.) The permanent teeth begin developing in the mandible during the first 6 months of life. The period of eruption of the mixed dentition occurs between 5 and 13 years of age, beginning with the eruption of the first permanent tooth. Exfoliation, or loss of the primary dentition, often begins with the central incisors and follows the eruption pattern. There are 32 permanent teeth (see Figure 13-7, B). Low birth weight, infection, and trauma have been associated with delayed eruption of the permanent teeth. Delayed exfoliation of the primary dentition has been associated with Down syndrome, hypothyroidism, osteogenesis imperfecta, and other congenital endocrine disorders. Dental enamel can be eroded, resulting in structurally weakened teeth in some conditions such as chronic gastroesophageal reflux disease, bulimia, and celiac disease. Dental caries are the most common chronic health condition in childhood.5 The infectious process of dental decay begins early in infancy when the bacterium Streptococcus mutans can be transmitted from parent or caretaker in the first few months of life. Ingestion of a high carbohydrate diet and/or frequent dietary sugars alters the oral bacterial composition, enhancing the development of dental caries in children and adolescents.6,7
Nose, mouth, and throat
Embryological development
Developmental variations
Age-Group
Physiological Variations
Newborn
Nose cartilage is soft, malleable; deformities in external appearance from intrauterine or birth positioning usually resolve spontaneously; congenital anatomic deformities, obstructive masses, or traumatic obstruction can occlude the nasal passages
Natal teeth may be present
Epstein pearls—small whitish nodules or cysts—at juncture of hard and soft palates may be visible in first month of life; Bohn nodules, or mucous gland cysts, may be present on gum surface in first 2 to 3 months
Rooting, gag, sucking reflexes are present
A short tight frenulum or frenulum attached to the inferior tip of the tongue may impede movement of the tongue and breastfeeding
Infancy
Anatomically small airway passages
Occlusion of nasal pathways can occur with nasal secretions
Deciduous teeth appear between 6 and 24 months
Rooting, sucking reflexes wane about 4 to 6 months
Drooling increases as salivary gland production increases
Anterior permanent teeth begin to calcify at 3 to 12 months
Ethmoid and maxillary sinuses present but undeveloped
Early childhood
Tonsils, adenoids enlarge and remain 2+ to 3+
Nasal passages enlarge allowing easier airflow
Maxillary and ethmoid sinuses present but sphenoid and frontal sinuses limited in size and function
Sinuses not normally assessed in children until middle childhood because of their limited development
Swallowing coordination improves; drooling decreases
Permanent molars begin to calcify at 18 months to 3 years
Middle childhood
Tonsils and adenoids usually begin to atrophy returning to size 1+ to 2+
Horizontal creases on anterior nose may develop in children with nasal rhinitis
Deciduous teeth begin to shed; permanent teeth erupt causing change in facial structure, appearance
Bridge of nose becomes more prominent
Third molar, last permanent tooth, is formed and begins calcifying
Adolescence
All permanent teeth present
Bridge of nose formed by bone creating pyramid shape
Frontal and sphenoid sinuses completely formed and functioning
Sinus Cavity
Development
Maxillary
Present at birth; first sinuses to develop significantly; can be seen radiologically at 4 to 5 months of age; opens beneath the middle turbinate into the middle meatus; rapid growth occurs between birth and 4 years of age and 6 to 12 years of age.
Frontal
Last sinuses to develop beginning between 4 and 8 years of age and do not develop fully until late adolescence. Secretions drain into the middle meatus. The walls of the frontal sinus border the orbital and intracranial cavities, increasing the risk for frontal sinus infections spreading directly into these adjacent structures.
Ethmoid
Present at birth, but not developed, grow rapidly during the first 4 years and are fully developed by 12 to 14 years of age; they are first seen radiologically at 1 year of age. Ethmoid sinuses are divided into anterior portion, draining into the middle meatus, and posterior portion, which drains into the superior meatus.
Sphenoid
Undeveloped at birth and do not begin to grow rapidly until 3 to 5 years of age; development complete between 12 and 15 years of age. They lie anterior to the pituitary fossa, and the optic nerve and carotid artery are located on the lateral wall of the sinuses offering a potential route for spread of infection into the central nervous system.
Anatomy and physiology
External nose
Internal nose
Nasopharynx
Sinuses
Mouth and oropharynx
Tonsils
Size
Description
1+
Tonsils visible slightly beyond tonsillar pillars
2+
Tonsils visible midway between tonsillar pillars and uvula
3+
Tonsils nearly touching the uvula
4+
Tonsils touching at midline occluding the oropharynx
Teeth
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Nose, mouth, and throat


Only gold members can continue reading. Log In or Register to continue
