Normal Skull Base Venous Variants
Christine M. Glastonbury, MBBS
DIFFERENTIAL DIAGNOSIS
Common
Jugular Foramen Asymmetry
Jugular Bulb Pseudolesion
Pterygoid Venous Plexus Asymmetry
Transmastoid Emissary Vein
Asymmetric Posterior Condylar Canal
Less Common
High Jugular Bulb
Jugular Bulb Diverticulum
Dehiscent Jugular Bulb
Asymmetric Sphenoidal Emissary Vein (of Vesalius)
Rare but Important
Foramen Cecum
Petrosquamosal Emissary Vein
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Intracranial venous flow must exit through skull base foramina
Normal structures may be asymmetric
Normal variants may be uni- or bilateral
Variants may be mistaken for masses, especially jugular foramen pseudolesion
MR pitfall results from variable signal intensity secondary to venous flow
Normal CECT ± normal bone CT clarifies
Asymmetric or enlarged veins may be sign of pathology
Helpful Clues for Common Diagnoses
Jugular Foramen Asymmetry
Key facts
Jugular veins usually asymmetric in size
Exaggerated asymmetry may result in larger side mimicking mass
More often MR pitfall
Imaging
MR: Unilateral high signal and enhancement
Look for ipsilateral enlarged transverse sinus
CECT: Normal jugular enhancement
Bone CT: Preservation of normal foraminal contours
Jugular Bulb Pseudolesion
Key facts
Turbulent venous flow creates MR pitfall
Asymmetric signal mimics pathology
Imaging
MR: Typically high signal intensity and avid enhancement
MRV or coronal T1 C+ usually clarify jugular bulb as normal
CECT: Normal jugular enhancement
Bone CT: Preservation of normal foraminal contours
Pterygoid Venous Plexus Asymmetry
Key facts
Unilateral prominence of deep facial veins that drain from cavernous sinus
Often incidental finding
Asymmetry may be pathological: Increased venous flow with caroticocavernous fistula
Imaging
CT: Curvilinear enhancement in medial masticator &/or parapharyngeal space
MR: Enhancement or flow voids in deep face, but no mass effect
Normal signal intensity of adjacent masticator muscles
Transmastoid Emissary Vein
Key facts
Transverse sinus to posterior auricular or occipital veins
Large veins may be pathological
Skull base dysplasia with small jugular foramina (e.g., achondroplasia)
Emissary and suboccipital veins “replace” jugular veins and are surgical hazard
Imaging
CECT: Enhancement of veins traversing mastoid bone
Bone CT: Smooth well-corticated channels through bone
Asymmetric Posterior Condylar Canal
Key facts
Synonym: Condyloid canal
Posterolateral to hypoglossal canal
Important channel for venous flow with atretic jugular veins
Contents: Meningeal branch of ascending pharyngeal artery; emissary vein from sigmoid sinus to suboccipital veins
Imaging
Bone CT: Well-corticated venous channel
CECT/MR C+: Venous enhancement
Helpful Clues for Less Common Diagnoses
High Jugular Bulb
Key facts
Usually incidental finding
May be associated with pulsatile tinnitus
Imaging
Axial bone CT: Bulb at level of cochlea
Coronal bone CT: Medial ± inferior to semicircular canals
MR: May be mistaken for unilateral mass because of high signal
MRV or coronal T1 C+ should clarify
Jugular Bulb Diverticulum
Key facts
Normal variant, incidental finding
May be associated with pulsatile tinnitus
Imaging
Bone CT: Best evaluated in coronal plane
Small “pouch” projecting from superior aspect of jugular bulb
MR: May be mistaken for temporal bone mass because of high signal
MRV or coronal T1 C+ should clarify
Dehiscent Jugular Bulb
Key facts
Otoscopy: “Vascular” middle ear mass
May be associated with pulsatile tinnitus
Absence of bony covering between jugular bulb and middle ear cavity
Imaging
CT: Absence of bony plate over jugular bulb at posterior hypotympanum
Asymmetric Sphenoidal Emissary Vein (of Vesalius)
Key facts
Synonym: Sphenoid emissary foramen
Transmits emissary vein from cavernous sinus to pterygoid venous plexus
Enlargement is pathological if ↑ venous flow from caroticocavernous fistula or tumor direct invasion
Imaging
May be partially assimilated with ovale or may be duplicated
Bone CT: Located medial to anterior aspect foramen ovale; usually < 2 mm
Helpful Clues for Rare Diagnoses
Foramen Cecum
Key facts
Usually closes during embryogenesis
Contains vein from sup sagittal sinus
Large foramen can be pathological
Suspect anterior neuropore anomaly
Imaging
Bone CT: Midline anterior to crista galli
Usually < 2 mm
Petrosquamosal Emissary Vein
Key facts
Embryonic venous remnant
Connects transverse sinus and retromandibular vein
Imaging
Bone CT: Vertical channel, ≤ 4 mm
Posterior to TMJ, anterior to EAC
Image Gallery
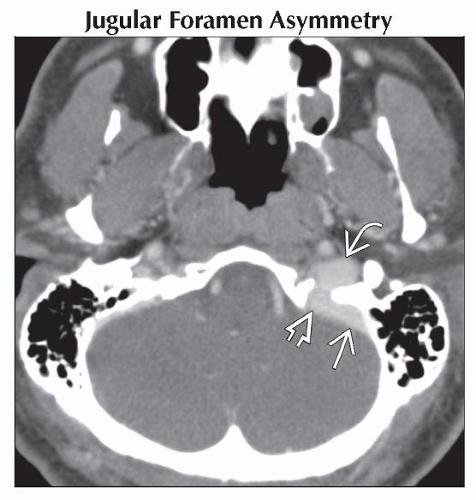 Axial CECT shows a normal left jugular foramen, though larger compared to the right. Note the left sigmoid sinus  , jugular foramen , jugular foramen  , and internal jugular vein , and internal jugular vein  are all significantly larger than the right. are all significantly larger than the right. |
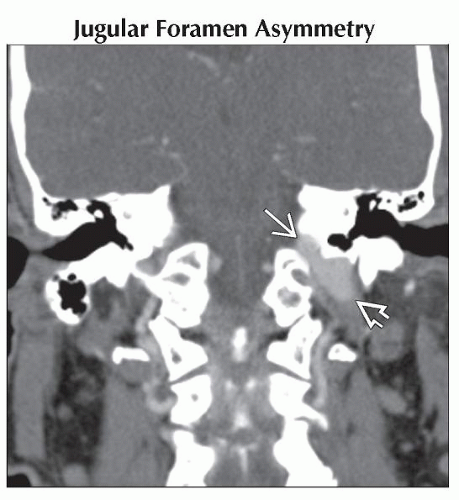 Coronal CECT in the same patient reveals the larger left jugular foramen  and internal jugular vein and internal jugular vein  . Such asymmetry is normal and does not imply underlying pathology. . Such asymmetry is normal and does not imply underlying pathology. |
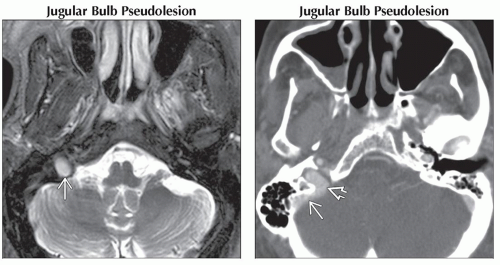 (Left) Axial T2WI FS MR performed during work-up of a possible metastatic disease reveals asymmetric hyperintensity in the right skull base  , which was intermediate intensity on T1 & enhanced with gadolinium (not shown). (Right) Axial CECT in the same patient reveals normal enhancement of the right sigmoid sinus , which was intermediate intensity on T1 & enhanced with gadolinium (not shown). (Right) Axial CECT in the same patient reveals normal enhancement of the right sigmoid sinus  & jugular bulb & jugular bulb  with normal foraminal contour. MR finding is attributed to turbulent venous flow in jugular foramen, not metastatic tumor. with normal foraminal contour. MR finding is attributed to turbulent venous flow in jugular foramen, not metastatic tumor. |
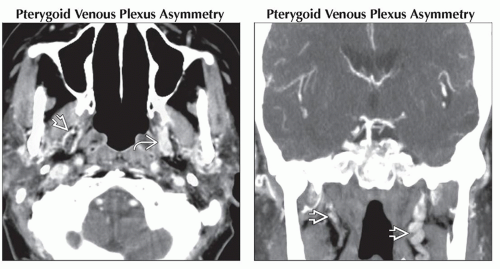 (Left) Axial CECT reveals curvilinear enhancement of the pterygoid venous plexus (PVP) bilaterally in the deep face. The right PVP
 has several linear vessels while the left has several linear vessels while the left  has a more prominent mass-like appearance. (Right) Coronal CECT in the same patient again shows asymmetry of the pterygoid plexus vessels has a more prominent mass-like appearance. (Right) Coronal CECT in the same patient again shows asymmetry of the pterygoid plexus vessels  in deep face. It also better illustrates the curvilinear vascular appearance of the plexus, confirming that this is not a true mass. in deep face. It also better illustrates the curvilinear vascular appearance of the plexus, confirming that this is not a true mass.Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|