Fig. 1.1
(a) Urogenital ridge and undifferentiated gonads. (b) Development of the gonads and Wolffian ducts in the male, and the Müllerian ducts in the female in (c). (d) Development of the genital ducts in the female. The formation of the uterine primordia and opening of the mesonephric ducts to the urogenital sinus is shown. (e) Lateral view showing the urorectal septum (URS) and the urogenital wedge (UW) (Taken from Acién and Acién [17], with permission)
The gonad is formed by the interaction between the primitive blastema in that area (somatic cells) and the gonocytes (germ cells) that migrate from the backside of the yolk sac. The somatic cells of the gonads are derived from mesonephric cells, which migrate into the area of the genital ridge early in development, and also from the mesenchyme and overlying coelomic epithelium [30]. The gonocytes or germ cells arrive at the gonadal ridge from the yolk sac, attracted by a chemotactic factor [71] or teloferon. In addition, there is a close association between the primordial germ cells and fibronectin and other components of the extracellular matrix during the migration [40]. Since the XX gonocytes arrive at the gonadal ridge later than the XY gonocytes (around the 10th–12th week), the wave of primary sexual cords has already passed and form the rete ovarii in the medullary region of the gonad. Now, in the absence of the Y chromosome, the male HY histocompatibility antigen and TDF/SRY gene (Sex-determining region of the Y chromosome gene) (but probably in the presence of HX antigen), the secondary sexual cords individually include each gonocyte in the cortical region of the gonad, generating primordial follicles and the cells of those cords differentiate into granulosa cells [8, 27]. Follicles fail to form in the absence of oocytes or with precious loss of germ cells, and oocytes not encompassed by follicular cells degenerate (Fig. 1.1).
The Internal Genitalia
The internal genitals begin their formation in the sixth week. In the thickness of the urogenital ridge, the mesonephric excretory tubules converge in a mesonephric or wolffian duct that descends to the cloacae in the urogenital sinus. Meanwhile, a longitudinal invagination of the celomic epithelium is formed on the outer side of the urogenital ridge and originates the paramesonephric or Müller’s duct. This one, at the top, opens into the celomic cavity, descends in parallel, and externally to the mesonephric duct, crossing it then ventrally, growing in the caudomedial direction until fusing and forming in the middle line a Y shape structure that is the uterine primordium, without reaching the urogenital sinus (Fig. 1.1).
Three portions can be distinguished in the müllerian ducts: a superior converging, a middle fused and an inferior diverging portion [72]. In any case, the most proximate part is the uterine isthmus at the internal cervical os level [13]. The lower diverging parts of these paramesonephric ducts fuse with the medial wall of the mesonephric ones inside a common basal membrane, and then, caudal to the end portion of the Müller ducts, over the dorsal wall of the urogenital sinus, an accumulation of paramesonephric cells which constitute the Müller tubercle [8] can be observed.
This Müller tubercle is then delimited laterally by the Wolff ducts [34, 43, 59]. These mesonephric or Wolffian ducts, close medially, do open into the urogenital sinus, and from the caudal tip of their opening, the ureteral buds sprout in each side and, growing laterally, anteriorly and cranially, move toward the metanephros to form the definitive kidney.
When the ovary is being formed, and therefore the testosterone and the AMH are absent, the Wolffian ducts become athretic and the Müllerian ones develop. The fused caudal parts of the paramesonephric ducts form the uterus, and the tubes come from the uppermost part that remains separated and opened into the celomic cavity. However, the adequate development and fusion of the paramesonephric ducts, the reabsorption of the middle septum and the correct formation of the normal uterus is induced by the laterally situated mesonephric ducts. The fusion and reabsorption processes begin at the uterine isthmus and progress simultaneously in both cranial and caudal directions [13, 67]. The mesonephric ducts act as guide elements for the paramesonephric ducts [43, 57].
The Müller tubercle’s cells remain below the uterus, and at both sides of it, a peritoneal fold which from the fused paramesonephric ducts move laterally towards the lateral walls of the bony pelvis, are known as the broad ligaments. The ovaries are located on the posterior surface of the broad ligaments.
The Urinary System
The development of the urinary system is intimately associated with that of the genital tract and occurs between the sixth and ninth week [67].
The metanephrogenic mass is formed in the intermediate mesoderm, caudally to the mesonephros, and is induced by the metanephric diverticulum or ureteral bud that has sprouted from the dorsal side of the mesonephric duct in its opening into the urogenital sinus. The ureteral bud forms the ureter and from its cranial part it expands to form the renal pelvis in the metanephrogenic mass.
The bladder and the urethra sprout from the urogenital sinus and adjacent mesenquima, though the ventrocraneal part of the bladder comes from the allantoids. After the division of the cloacae by the urorectal septum, the formation of the rectum and superior anal duct dorsally and urogenital sinus ventrally occurs [56]. In the inferior part of the urogenital sinus, in front of the urorectal septum, the mesonephric ducts open, and the bladder is formed ventrally which incorporates the allantoids. Gradually, the bladder ascends and the most caudal part of the mesonephric ducts with the ureteral bud (what has been named the “Wolffian patch” – [72]) ends up incorporated into the dorsal wall. Like this, the ureters are incorporated and remain, opening themselves separately, in the adult vesical trigone.
Now, the growing of a new urogenital fold (the urogenital wedge) finally separates the bladder and the urethra anterior and ventrally, while the mesonephric ducts continue opening into the lower side of the urogenital sinus (Fig. 1.2).
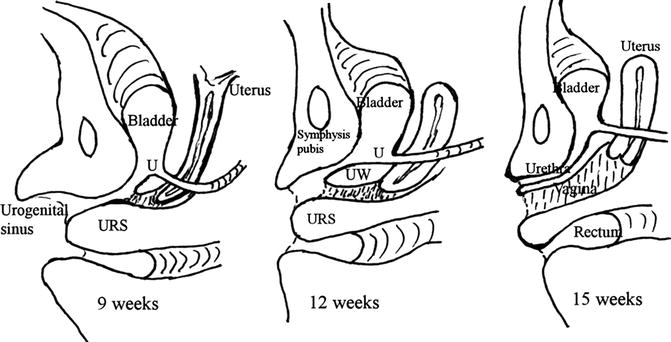
Fig. 1.2
Development of the urogenital sinus from 9 to 15 weeks. U ureter, UW urogenital wedge, URS, urorectal septum (Taken from Acién and Acién [17], with permission)
The Vagina
The vagina is the female genital organ whose embryology is more controversial. There are theories that suggest it derives from the paramesonephric ducts [47, 75], from the mesonephric or Wolffian ducts [38], from the urogenital sinus [63], or from a combination of these structures [60, 62]. Until very recently, the most generalized theory about the embryology of the vagina suggested that its upper part comes from the Müller ducts (müllerian vagina) and the lower part from the urogenital sinus (sinus vagina) [33, 67], though always assuming the inducing function of the mesonephric ducts in the appropriate müllerian development [43, 57].
However, apart from the inducing role of the mesonephric ducts on the Müllerian ducts, different studies, some of them experimental, have proved their participation in the formation of the vagina, so that the “protrusions of the sinus” or the “sinuvaginal bulbs” observed during the development of the vagina would actually be the caudal segments of the Wolffian ducts [28, 29, 37, 60]. Certainly, Hart [46] had already adopted the term “Wolffian bulb” because the epithelial pockets that form the sinuvaginal bulbs keep remnants of the wolffian ducts. Witschi [76] re-examined the Koff’s embryo and deduced that the sinuvaginal bulbs were identical to the lower segments of the Wolffian ducts. This observation was confirmed by Bok and Drews [28] in an experimental study with embryo cultures.
These findings, together with the analysis of published papers [23, 36, 41, 49, 61, 68, 70], as well as cases studied by us [1–4, 6, 7], especially those referring to patients with renal agenesis and ipsilateral blind hemivagina, led to our proposal of an embryological hypothesis [3, 8]: “The vagina seems to come completely from the fused mesonephric ducts, though the Müller tubercle would also take part and is fundamental for its adequate formation and cavitation”.
According to this embryological hypothesis, the fused Müller ducts would form the uterus until the external cervical orifice, induced by the mesonephric ducts that descend at both sides and to which they caudally fuse after their divergence. Later, the mesonephric ducts regress cranially but from the level of the external cervical os, they enlarge and form the sinuvaginal bulbs, incorporating the Müller tubercle’s cells to the vaginal plate formed by the fusion of both bulbs (Fig. 1.3). Likewise, the Müller tubercle would be delimited at the top and laterally by the diverging portion of the Müller ducts, more laterally by the Wolffian ducts, infero-laterally by the portion of the sinuvaginal bulbs and below by the urogenital sinus [72].
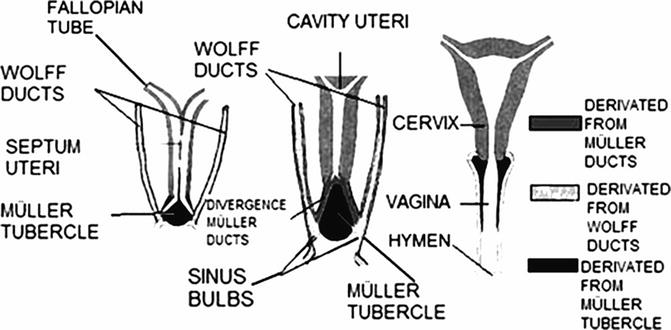
Fig. 1.3
Representative diagram of the evolution of the Wolffian and Müllerian ducts, the Müller tubercle and the formation of the vagina, according to the studies of Acién and Sánchez-Ferrer (Taken from Acién and Acién [17], with permission)
The posterior cavitation of the Müller tubercle lets the müllerian cells cover the primitive vaginal cavity with a cuboidal or paramesonephric epithelium. Then, by metaplasic induction or, more probably, by epidermization from the urogenital sinus, the vagina becomes lined by a flat, squamous, polystratified epithelium. Some mesonephric remnants may remain in the vaginal wall, which occasionally can give rise to Gartner cysts.
This hypothesis has also been proved experimentally in rat embryos by our group [72], as we observed that the protrusions of the sinus or the sinuvaginal bulbs are positive for specific inmunohistochemical markers for wolffian derivatives (GZ1 and GZ2) and that in posterior stages of the development, these markers show themselves all along the completely formed vagina.
Since the ureteral bud sprouts from the opening in the urogenital sinus of the mesonephric duct, the absence or distal injury of a duct would mean the absence of the ureteral bud and, therefore, the definitive kidney would not develop either, which will result in renal agenesis in that side and in blind or ipsilateral athretic hemivagina. In these cases, mesonephric and paramesonephric remnants are frequently found in the intervaginal septum and are identified as such by the characteristics of the epithelium that lines them [5, 7, 74].
Suidan and Azoury [74] pointed out that the epithelium of the vagina and of the transverse vaginal septum are from a mesonephric origin. Certainly, the epithelium that covers the blind hemivagina has müllerian characteristics (cuboidal) [45, 68] except when there is some communication with the permeable side or inflammation; in these cases, it is epidermoid, squamous, stratified and flat. And when the blind vagina is athresic, small, found in the anterolateral upper part of the normal hemivagina and lateral to the cervix (Gartner pseudocyst, Herlyn-Werner Syndrome and Wunderlich Syndrome), then the epithelium is of a mesonephric kind, probably due to the absence or non-participation of the Müller tubercle [4, 5, 7].
Besides, in cases of blind hemivagina there is generally an associated uterine malformation (normally a duplicity) because of a failure in the inducing function of the injured mesonephric duct.
The External Genitalia
The development of the external genitalia begins in the fourth week with the formation of the genital tubercle in the ventral portion of the cloacal membrane, but the final aspect is not established until the 12th week. Genital swellings and urogenital or urethral folds appear on each side soon after, and between both folds is the urogenital groove and membrane.
The genital tubercle forms the phallus, which in absence of male inductors becomes the clitoris, while the genital folds form the labia majora. The urogenital or urethral folds do not fuse and form the labia minora. The urogenital groove remains open hence forming the introitum, where the urethra, and later the vagina, will open after the fenestration of the urogenital membrane; and the remnants of that membrane will be the hymen [51].
The Gubernaculum
The gubernaculum forms from the caudal fold that provokes the mesonephros elevating the covering peritoneum (Fig. 1.4). It begins as a cord that extends from the gonadal ridge, to the future inguinal region and its insertion into the urogenital cord differentiates two portions of the Müller duct [18, 49].
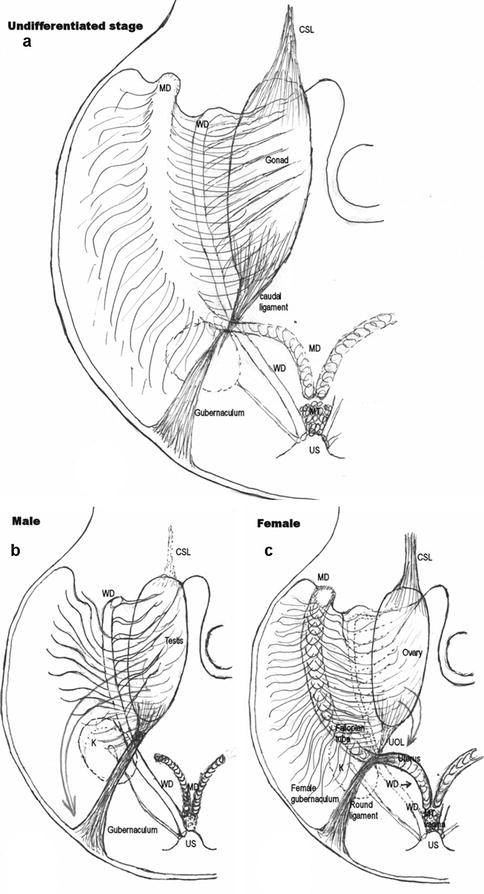
Fig. 1.4
Schematic illustration of the possible development of the gubernaculum. (a) At an Undifferentiated stage. (b) In Males. (c) In Females. CSL cranial suspensory ligament, WD wolffian duct, MD müllerian duct, MT müllerian tubercle, US urogenital sinus, K kidney, UOL uteroovarian ligament (caudal ligament of the gonad) (Taken from Acién et al. [18], with permission)
In the absence of testicular differentiation that is, in the absence of androgens and AMH and presence of ovary formation, the paramesonephric or Müllerian ducts complete their invagination and development, interfering the connection of this tissular column that has arisen from the inguinal cone with the mesonephric duct and the caudal ligament of the gonad. The gubernaculum then grows over the paramesonephric ducts, and its muscular fibres incorporate into the wall of the Müllerian ducts, becoming the round ligament. Behind and above, in the absence of androgens and AMH, only athretic remnants of the mesonephric duct remain; thus, the caudal ligament, uniting the gonad inferior pole to the posterior wall of the Müllerian ducts, constitutes the utero-ovarian ligament.
The Müllerian ducts continue their development, and induced by the mesonephric ducts, complete the fusion process, the reabsorption of the middle septum and the appropriate formation of the uterus. It remains unclear whether the growth of the female gubernaculum and its fusion with the developing Müllerian ducts could be one of the most important processes in the induction of the formation of the uterus, but it has been suggested that a gubernaculum anomaly could lead to certain genital malformations and a fusion defect between the müllerian ducts [14, 18, 19].
The interaction and correspondence between the analysed embrionary structures and its normal or abnormal adult derivates is shown in Table 1.1.
Table 1.1
Adult derivatives and female abnormalities of embryonic urogenital structures
Embryonic structure | Normal derivatives | Female abnormalities |
|---|---|---|
Urogenital ridge with mesonephros and mesonephric ducts (Wolffian ducts) opening to urogenital sinus | 1. Epoophoron, paroophoron (paraovarian cysts), mesonephric duct remnants (Gardner cysts) | 1. Agenesis of all derivatives of one urogenital ridge (ovary, tube, hemiuterus, and kidney): unilateral renal agenesis and contralateral unicornuate uterus |
2. Ureteral bud (ureter, pelvis, calyces, and collecting tubules): normal kidney
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|