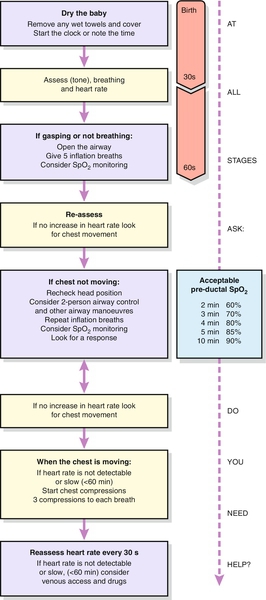
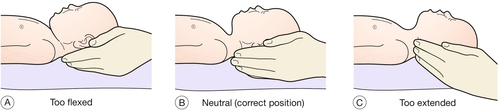
49 Clamping of the cord after delivery leads to acute hypoxia. This is thought to be the major stimulant for a baby to start breathing. Physical stimuli such as cold air, rubbing or physical discomfort may also provoke respiratory efforts. If the baby fails to start breathing, the baby’s oxygen concentration falls further, the baby loses consciousness and enters ‘primary apnoea’. After 5–10 min of primary apnoea, spinal centres, which are normally suppressed by higher centres, begin to cause shuddering of the baby’s body at a rate of approximately 12/min (agonal gasps). Once this gasping stops, the baby enters ‘secondary’ (or ‘terminal’) apnoea and without intervention, the outcome is death. The only way to tell whether a non-breathing newborn infant is in primary or secondary apnoea is by assessment of its response to resuscitation. If in primary apnoea, nearly all infants will start breathing within a few breaths; if secondary, the baby will usually gasp for some time before starting regular respiration. In reality, however, both are initially managed in the same way. Most babies born in primary apnoea will breathe spontaneously within 60–90 s given a clear airway. The basic approach to all resuscitation is therefore Airway, Breathing and Circulation (ABC). Dry the baby immediately and then wrap in a warm dry towel. A naked, wet baby can still become hypothermic despite a warm room, especially if there is a draught. Cold babies have an increased oxygen consumption and are more likely to become hypoglycaemic and acidotic. Babies also have a large surface area-to-weight ratio and heat can therefore be lost very quickly. Most of the heat loss is by evaporation and outcome is therefore improved by drying (Fig. 49.1). Position the baby with the head in the neutral position. Overextension may collapse the newborn baby’s pharyngeal airway, just as will flexion (Fig. 49.2). A folded towel placed under the neck and shoulders may help to maintain the airway in a neutral position and a jaw thrust may be needed to bring the tongue forward and open the airway, especially if the baby is unresponsive. Meconium-stained liquor is relatively common. Fortunately, meconium aspiration is a rare event and often occurs in utero before delivery. If the baby is active, no specific action (other than drying and wrapping the baby) is needed. If the baby is not active, inspect the oropharynx with a laryngoscope and aspirate any particulate meconium seen using a soft catheter under direct vision of the vocal cords. Action points if no response:
Neonatal resuscitation
Physiology
Practical aspects of neonatal resuscitation
Dry, wrap and keep the baby warm
Airway
 Is the baby in the neutral position?
Is the baby in the neutral position?
 Is there a good seal on the mask?
Is there a good seal on the mask?
 Do you need to perform a jaw thrust?
Do you need to perform a jaw thrust?
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


