24 Examination for genital infections Taking samples for genital infections Symptoms associated with genital infections Genital infections in females can be caused by infections such as bacterial vaginosis and Candida albicans that are not sexually transmitted, are common and do not usually have serious sequelae, or by sexually transmitted infections (STIs). STIs including Chlamydia trachomatis, syphilis and genital herpes can cause long-term morbidity. In women, untreated infections can lead to chronic pain or infertility and may significantly increase susceptibility to sexual transmission of HIV. The World Health Organization (WHO) identifies unsafe sex as the second most important cause (after being underweight) of ill-health in the world, causing 17% of all economic losses through ill-health in the developing countries. It estimates that there are over 340 million cases of the four major curable STIs (syphilis, gonorrhoea, chlamydia and trichomoniasis) in adults aged 15–49 throughout the world each year; 90% in developing countries. The Joint United Nations Programme on HIV/AIDS (UNAIDS) estimated that at the end of 2010, 34 million adults and children were living with HIV/AIDS worldwide. The incidence of new HIV infections is around 2.7 million per year, down 21% from a peak in the late 1990s. There is cause for cautious optimism: 6.6 million people (about half of those who require it) were receiving antiretroviral therapy at the end of 2010, with an estimated 2.5 million deaths and 350 000 vertical transmissions to children averted through treatment since 1995. The main burden of the epidemic is felt in sub-Saharan Africa, where three women are newly infected to every two men. Nonetheless, in 22 African countries, HIV incidence fell by more than a quarter over the decade to 2010 and African women are more likely to access antiretroviral therapy than their male counterparts. There have been dramatic changes in the pattern of STI over the past 50 years. In the UK, there was a decline in syphilis following the end of the Second World War, and in gonorrhoea from the 1970s, until the 1990s. However, during this time, there was an increase in chlamydia, herpes, wart virus and HIV infections. From the mid-1990s, the downward trend in the bacterial STIs then reversed, and viral STIs continued to increase. Cases of chlamydia, genital herpes and genital warts have continued to rise in both men and women, but gonorrhoea rates peaked in 2002 and have then steadily declined. A dramatic rise in cases of syphilis between 2000 and 2006 was largely attributable to cases in men, particularly men-who-have-sex-with-men, although there was a 438% rise in cases in women. Syphilis diagnoses then declined slowly but remain a concern – untreated syphilis in early pregnancy leads to a stillbirth rate of 25%. The number of diagnoses of HIV in the UK peaked in 2005 and has since fallen slightly, to around 6000 cases per year. However the number acquired within the UK almost doubled between 2001 and 2010 and now exceeds the total acquired abroad. Rises in STI diagnoses in women have been greatest in those aged 15–19 years, and have continued despite advances in prevention and treatment. Contributory factors include changes in sexual behaviour, early sexual debut, increased geographical mobility within and between countries, the emergence of drug-resistant strains, symptomless carriers, lack of public education, the reluctance of some patients to seek treatment and barriers to accessing testing and treatment services affecting those most at risk of infection. The risk of STI acquisition is increased with younger age (under 25), prior STI diagnosis, frequent partner change or concurrent partners, non-use of condoms and high rates of condom errors. A number of groups including individuals who misuse drugs or alcohol; looked after and accommodated adolescents; sex workers; prisoners; those with sexual compulsion and addiction; and those with learning disabilities or poor mental health are often regarded as having high risk of STI. Although definitive evidence for increased STI prevalence is mixed or lacking, clinicians maintain a low threshold for STI testing in these groups. For many women, particularly in developing countries, it is the social and demographic risk factors affecting the community from which she chooses a regular partner, rather than her own individual risk factors, that determine STI risk. Most STIs are asymptomatic and only a small proportion of women who present with symptoms such as vaginal discharge have an STI. Conversely, about 70% of women with chlamydia, 50% with gonorrhoea, 65% with pelvic inflammatory disease (PID), 30% with genital warts and 50% with genital herpes, have no symptoms. Hence, performing STI testing solely in all women who present with genital symptoms will result in large numbers of tests being performed on women at very low risk of STI, but miss or delay a diagnosis in women at risk both of serious complications and of onward horizontal and vertical transmission of infection. Opt-out testing for HIV and syphilis infection are routine parts of antenatal care in the UK, and the English National Chlamydia Screening Programme tested over 2 million young men and women in 2011, diagnosing almost 150 000 chlamydial infections. These population-level interventions, along with vaccination for HPV (human papillomavirus) and opportunistic testing for infections have had some impact on the prevalence of infection and the rate of serious sequelae. In routine clinical practice, the risk of adverse outcomes is reduced by maintaining a low threshold for performing tests in both symptomatic and asymptomatic women, a high level of awareness of the genital and non-genital manifestations of STI and above all, routinely including a risk assessment in clinical history-taking. For example, routine questions confirming a history of sex with partners from groups with elevated HIV prevalence, such as those of African origin, in a woman presenting for the treatment of cervical intraepithelial neoplasia, might result in an early diagnosis of HIV infection, significantly extending life expectancy. Once an STI has been diagnosed, partner notification (contact tracing) is essential in the management of HIV and bacterial STIs both to prevent reinfection in those that are curable and to avoid further onward transmission. Partner notification strategies include: patient referral, where the patient informs recent partner(s); provider referral, where details are passed to a healthcare professional who then contacts the partners; and conditional referral, where provider referral is initiated if patient referral has not occurred after an agreed period has elapsed. In provider referral it is usual to protect the identity of the index patient. Enhanced partner notification strategies include providing the patient with antibiotic treatment for the partner or with a pharmacy voucher for treatment and the use of innovative web applications or mobile apps to allow patients to inform partners, while preserving anonymity, is increasing. Patients are advised to abstain from sex until they and their partner(s) have completed treatment. A follow-up consultation (in person or by phone) may be performed after treatment to check that medication has been completed, that there has been sexual abstinence, and that the partner(s) has been treated. The need to accurately assess risk factors and to sensitively and appropriately identify current and previous partners makes good sexual history-taking a critical factor in STI management. A woman who is complaining of genital symptoms expects to be asked questions related to this, but may or may not have considered the possibility of an STI. Asymptomatic women attending for other reasons, such as termination of pregnancy, may also be unaware of STI risk. Time, sensitivity and privacy must be ensured: interviews should take place in a soundproof setting. Accurate answers to a risk assessment may not be possible with a partner or relative present. Questioning should be sensitive, inclusive and appropriate, but direct, avoiding euphemisms. As with all history-taking, choice of words, and appropriate facial expressions and body language in the questioner are important. Use open language to avoid conveying any impression of being judgemental; examples are the use of inclusive words such as ‘partner’ rather than ‘boyfriend’. Permission-giving might involve providing a selection of possible answers to a question that includes those which might be judged socially or morally unacceptable, such as non-use of condoms or anal intercourse. Carefully introducing subjects or words that the patient might find difficult, the words ‘consent’ and ‘rape’ for example, can help with disclosure. The history-taking should start by asking about the presenting complaint. An open question followed by more open questions is usually the best approach. A small number of direct closed questions will often clarify details of vaginal discharge, dysuria, vulval lumps, ulcers or lower abdominal pain. Supplementary questions about these symptoms are given below. The patient should then be asked about her gynaecological history. The final part should be the sexual history, in order to assess the risk of STIs. ‘When did you last have sex?’ is often entirely acceptable, but asking ‘Do you have a (sexual) partner?’ can be a gentler introduction if the woman is not expecting questions about sexual contacts. This can lead to questions about the woman’s most recent sexual exposure: Asking about ‘previous’ sexual partners immediately conveys an expectation of serial monogamy, making it even harder for a woman to disclose a concurrent partner. Around 9% of sexually active women in the UK report a concurrent sexual partnership in the previous year. Supplementary questions about risk of exposure to HIV infection should also be asked. Clinical symptoms are not helpful at indicating the site of infection and are of limited use in determining which infection is likely to be present. Examination should be performed in all women with symptoms. This should be in a private room and the woman should be provided with a gown to cover the areas not being examined. All women should be offered a chaperone for both the history and examination, regardless of the practitioner’s gender. It is essential that all males have a chaperone when examining a woman’s genital tract. Ensuring that the patient is in a comfortable position, and understands what the examination and any samples taken will involve, will make the procedure easier for both patient and clinician. The woman should be in the lithotomy position, and there should be a good light source behind the examiner. The following genital examination should be performed: Syndromic management, based on a combination of clinical symptoms and signs, is appropriate for women at low risk of STI who present with a first episode of uncomplicated vaginal discharge. In most other cases, samples for microbiological testing will be required. It is important that swabs are performed adequately and that the specimen is placed in the appropriate culture or transport medium. The samples required and the infections being tested for should be explained to the patient and informed consent obtained. Nucleic acid amplification testing (NAAT) is increasingly available for the diagnosis of chlamydia, gonorrhoea, herpes simplex, and, less commonly, syphilis and trichomoniasis and has simplified obtaining, transporting, storing and analysing specimens for STI diagnosis. For routine testing for chlamydia and gonorrhoea in asymptomatic women, or where genital examination is not possible, a self-obtained vulvovaginal swab for NAAT testing has comparable sensitivity and specificity to physician obtained samples. When samples for culture or microscopy are required, or during the examination of a symptomatic woman, the swabs required will depend on the laboratory facilities available locally, and the symptoms. Assessment may include the following: Many infections are completely asymptomatic, so testing should be considered on the basis of risk factors. An increase in vaginal discharge may be due to a number of infective and non-infective conditions (Table 24.1). Even in areas of high STI prevalence, the great majority of women presenting with vaginal discharge will not have an STI. Physiological discharge can only be diagnosed after negative swabs have excluded the infective causes. Questions that help distinguish between the causes are: Dysuria is usually due to acute bacterial cystitis, urethritis or vulvitis (Table 24.2). External dysuria, particularly in the absence of frequency or abdominal pain, indicates irritation at the urethral meatus. Questions that help distinguish between the causes are: Raised lesions on the vulva can be due to infections or anatomical variants. Genital warts are by far the most common cause of vulval lumps (Table 24.3). Questions that help distinguish between the causes are: Infective lesions are the most common cause of vulval ulcers, with genital herpes being the main infection in the UK (Table 24.4). Questions that help distinguish between the causes are:
Sexually transmitted infections
Introduction
Principles of STI management
Sexual history
 How long ago was it?
How long ago was it?
 Was this with a regular partner, a one-off encounter or something else?
Was this with a regular partner, a one-off encounter or something else?
 If a regular partner, for how long?
If a regular partner, for how long?
 Was it a man or a woman?
Was it a man or a woman?
 What kind of contraception/protection was used?
What kind of contraception/protection was used?
 If condoms were used, were they used consistently and properly, and have there been any recent breakages?
If condoms were used, were they used consistently and properly, and have there been any recent breakages?
 Has the sexual partner got any genital symptoms?
Has the sexual partner got any genital symptoms?
Other sexual partners
 When did she last have sex with a different partner? If within the past few months, the same details as above need to be obtained.
When did she last have sex with a different partner? If within the past few months, the same details as above need to be obtained.
 How many different partners have there been over the past few months?
How many different partners have there been over the past few months?
Assessment of HIV risk
 Have any partners been from areas where HIV is more common, such as sub-Saharan Africa and Asia?
Have any partners been from areas where HIV is more common, such as sub-Saharan Africa and Asia?
 Has she ever injected drugs?
Has she ever injected drugs?
 Are any male partners known to be bisexual or injecting drug users.
Are any male partners known to be bisexual or injecting drug users.
Examination for genital infections
 inspect the pubic hair and surrounding skin for pubic lice and any skin rashes
inspect the pubic hair and surrounding skin for pubic lice and any skin rashes
 palpate the inguinal region for lymphadenopathy
palpate the inguinal region for lymphadenopathy
 inspect the labia majora and minora, clitoris, introitus, perineum and perianal area for warts, ulcers, erythema or excoriation
inspect the labia majora and minora, clitoris, introitus, perineum and perianal area for warts, ulcers, erythema or excoriation
 inspect the urethral meatus and Skene’s (see History box) and Bartholin’s glands for any discharge or swelling
inspect the urethral meatus and Skene’s (see History box) and Bartholin’s glands for any discharge or swelling
 insert a bivalve speculum into the vagina
insert a bivalve speculum into the vagina
 inspect the vaginal walls for erythema, discharge, warts, ulcers
inspect the vaginal walls for erythema, discharge, warts, ulcers
 inspect the cervix for discharge, erythema, contact bleeding, ulcers or raised lesions. Mucopurulent discharge from the cervix is not a reliable indicator of infection
inspect the cervix for discharge, erythema, contact bleeding, ulcers or raised lesions. Mucopurulent discharge from the cervix is not a reliable indicator of infection
 perform a bimanual pelvic examination to assess size and any tenderness of the uterus, cervical motion tenderness (cervical excitation) and adnexal tenderness or masses.
perform a bimanual pelvic examination to assess size and any tenderness of the uterus, cervical motion tenderness (cervical excitation) and adnexal tenderness or masses.
Taking samples for genital infections
 a urethral swab for culture for gonorrhoea placed in Amies, Stuart’s or similar transport medium
a urethral swab for culture for gonorrhoea placed in Amies, Stuart’s or similar transport medium
 observe the vaginal discharge to see if it has the homogeneous, white appearance typical of bacterial vaginosis
observe the vaginal discharge to see if it has the homogeneous, white appearance typical of bacterial vaginosis
 swab the lateral vaginal walls and the pool of discharge in the posterior fornix. Smear some of the discharge onto a glass slide and allow to air dry (for Gram-staining by the laboratory for clue cells, pseudohyphae and spores)
swab the lateral vaginal walls and the pool of discharge in the posterior fornix. Smear some of the discharge onto a glass slide and allow to air dry (for Gram-staining by the laboratory for clue cells, pseudohyphae and spores)
 test the pH of the vaginal discharge either by touching the swab used to take the vaginal specimen onto narrow-range pH paper, or the paper can be pressed against the lateral vaginal walls with sponge holders. It is important that cervical secretions are avoided for this, as cervical mucus has a pH of 7 and any contamination will give a falsely high reading
test the pH of the vaginal discharge either by touching the swab used to take the vaginal specimen onto narrow-range pH paper, or the paper can be pressed against the lateral vaginal walls with sponge holders. It is important that cervical secretions are avoided for this, as cervical mucus has a pH of 7 and any contamination will give a falsely high reading
 any vaginal secretions should be wiped from the cervix
any vaginal secretions should be wiped from the cervix
 an endocervical swab for identification of gonorrhoea (into a commercial medium for gonococcal nucleic acid amplification testing, or for culture placed in Amies, Stuart’s or similar transport medium with the urethral swab)
an endocervical swab for identification of gonorrhoea (into a commercial medium for gonococcal nucleic acid amplification testing, or for culture placed in Amies, Stuart’s or similar transport medium with the urethral swab)
 an endocervical sample for chlamydia nucleic acid amplification testing (in most cases a single swab is used for both chlamydia and gonorrhoea NAAT)
an endocervical sample for chlamydia nucleic acid amplification testing (in most cases a single swab is used for both chlamydia and gonorrhoea NAAT)
 a blood sample for syphilis serology
a blood sample for syphilis serology
 a blood sample for hepatitis B testing if the woman or any of her sexual partners are from areas of high hepatitis B prevalence (e.g. sub-Saharan Africa or Asia)
a blood sample for hepatitis B testing if the woman or any of her sexual partners are from areas of high hepatitis B prevalence (e.g. sub-Saharan Africa or Asia)
 a blood sample for hepatitis B and C testing, if the woman or any of her sexual partners have ever injected drugs
a blood sample for hepatitis B and C testing, if the woman or any of her sexual partners have ever injected drugs
 hepatitis B immunization if the hepatitis B test is negative and she is at continued risk
hepatitis B immunization if the hepatitis B test is negative and she is at continued risk
 a blood sample for HIV testing
a blood sample for HIV testing
 if vesicles, ulcers or fissures are seen, a sample for herpes culture should be taken from the base of the lesion and sent to the laboratory in viral transport medium.
if vesicles, ulcers or fissures are seen, a sample for herpes culture should be taken from the base of the lesion and sent to the laboratory in viral transport medium.
Symptoms associated with genital infections
None
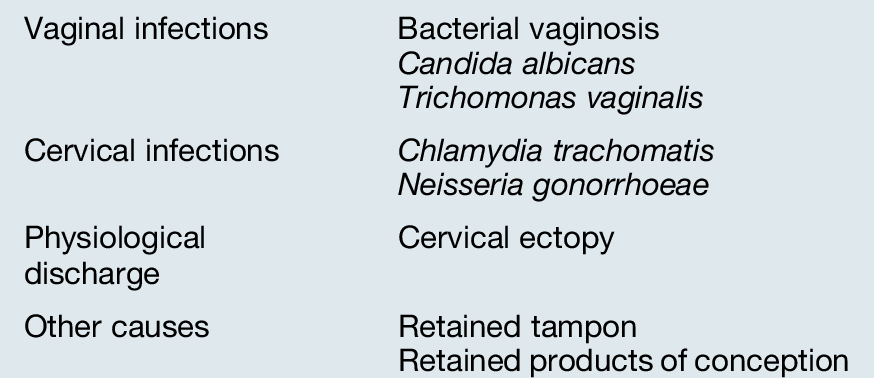
Vaginal discharge
 Does the discharge have an offensive odour?
Does the discharge have an offensive odour?
 Is there any vulval itching or soreness?
Is there any vulval itching or soreness?
 Are there any other symptoms such as dysuria, intermenstrual or postcoital bleeding or abdominal pain?
Are there any other symptoms such as dysuria, intermenstrual or postcoital bleeding or abdominal pain?
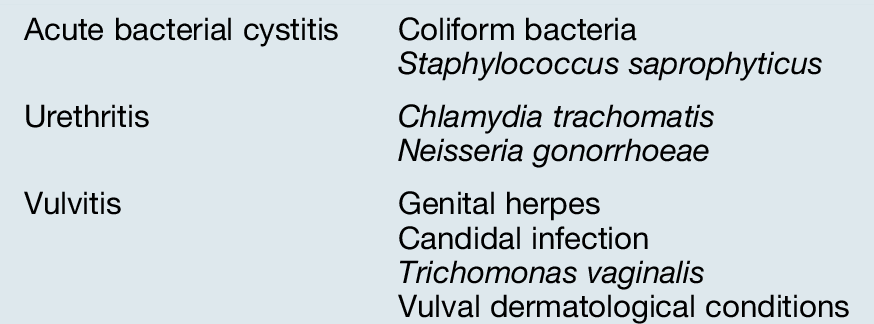
Dysuria
 Is the dysuria external, i.e. is it as the urine comes into contact with the vulval mucosa?
Is the dysuria external, i.e. is it as the urine comes into contact with the vulval mucosa?
 Is there any urinary frequency, nocturia or haematuria?
Is there any urinary frequency, nocturia or haematuria?
 Is there any vaginal discharge, post-coital or intermenstrual bleeding or abdominal pain?
Is there any vaginal discharge, post-coital or intermenstrual bleeding or abdominal pain?
 Are there any vulval sores or itching?
Are there any vulval sores or itching?
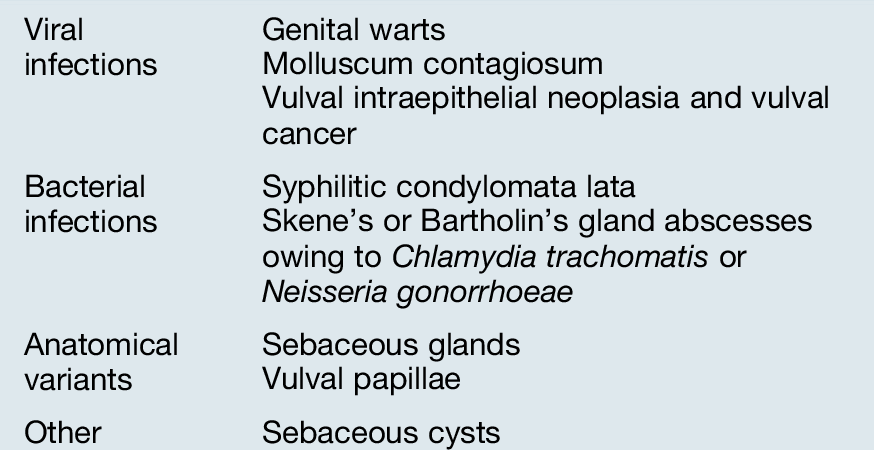
Vulval lumps
 Are the lumps painful?
Are the lumps painful?
 How many are there?
How many are there?
 How long have they been present?
How long have they been present?
 Are there any other symptoms such as dysuria, intermenstrual or post-coital bleeding or abdominal pain?
Are there any other symptoms such as dysuria, intermenstrual or post-coital bleeding or abdominal pain?
Vulval ulcers
 Are the ulcers painful?
Are the ulcers painful?

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


