Fig. 22.1
Diagnosis of neonatal intestinal obstruction
Differential Diagnosis
Atresia and stenosis involving duodenum, small bowel, and colon
Intestinal malrotation
Meconium ileus (associated and not associated with cystic fibrosis)
Hirschsprung’s disease (HD)
Small left colon
Meconium plug syndrome
Volvulus, internal herniation
Late-presenting cases of anorectal malformations (ARM)
Necrotizing enterocolitis (NEC)
Rare causes include:
Large retroperitoneal masses
Intussusception
Missed (late presenting) obstructed inguinal hernia
Remember to exclude nonsurgical causes of abdominal distension .
Presentation
“A neonate with bilious vomiting or aspirate has intestinal obstruction until proved otherwise.”
The presenting symptoms could be any combination of the following:
Bilious vomiting
Abdominal distension (Fig. 22.2)

Fig. 22.2
A newborn with marked abdominal distension suggesting distal intestinal obstruction, necrotizing enterocolitis, or sepsis. The more marked the abdominal distension, the more distal is the obstruction
Delayed passage of meconium
Passage of grayish white pellets only
Sepsis
History should include :
Length of pregnancy
Antenatal (presence of polyhydramnios may indicate intestinal obstruction) and family history (relevant in cases of HD and cystic fibrosis)
Maternal diabetes (relevant in cases of small left colon syndrome)
Passage of meconium (assisted or unassisted) and its timing (delayed passage of meconium beyond 24 h is a presenting symptom of HD or small left colon syndrome and needs to be investigated)
Passage of a plug of meconium
If the baby has passed anything rectally? If yes, color and consistency of the content (in intestinal atresia the baby may pass greenish white pellets)
Results of antenatal ultrasound (dilated bowel loops indicating bowel obstruction)
Examination
In the examination, look for and note:
The presence of a normal anus (Fig. 22.3).

Fig. 22.3
A clinical photograph showing absent anus diagnostic of anorectal malformation
A normal anus may be seen in cases of congenital rectal atresia (Fig. 22.4).
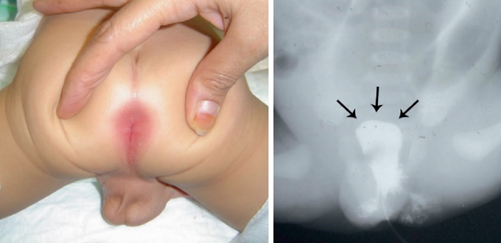
Fig. 22.4
A clinical photograph showing a normal looking anus in a newborn with congenital rectal atresia confirmed by barium enema
Extent of abdominal distension , if any.
No distension with duodenal obstruction.
Early and upper abdominal distension with proximal intestinal obstruction.
With more distal obstruction distension is generalized and slow to appear.
Visible and palpable bowel loops.
Erythema and tenderness of abdominal wall (denotes NEC with perforation or gangrene of bowel or volvulus. It may also be seen in cases of a meconium cyst).
Extent of dehydration (judged by reduced urine output, dryness of tongue, sunken fontanels).
Associated anomaly (e.g., Down’s syndrome can be a pointer to duodenal atresia or HD).
Investigations
Complete blood count (CBC).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


