Problem
Cesarean hysterectomy for placenta percreta has the potential for significant hemorrhage. Commonly a classical hysterotomy is created and this can often result in a 500-800 mL blood loss before the hysterectomy even begins. Theoretically, an almost bloodless cesarean delivery may reduce the blood loss for the entire procedure, avoiding significant crystalloid/colloid infusion and/or blood product transfusion despite as much as a 1500 mL blood loss at the time of hysterectomy.
Our solution
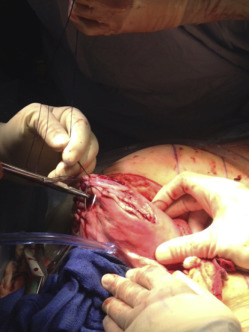
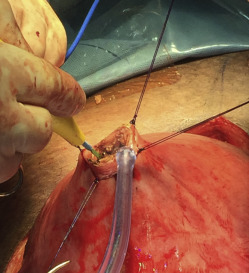
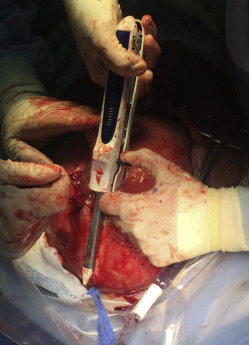
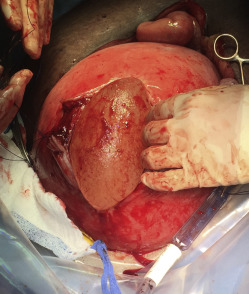
A midline abdominal incision allows exteriorization of the pregnant uterus. The site for the upper segment hysterotomy is identified (usually high on the upper segment and fundus) in an area free of scarring. The uterine wall is initially grasped between thumb and forefinger to create a fold of uterus in which no part of the fetus or umbilical cord is located ( Figure 1 and Video ). In a placenta previa percreta this is done in the uterine fundus (anteriorly or posteriorly) and as far away from the placenta as possible. Four full-thickness no. 1 polydioxanone interrupted sutures (PDS-II, Ethicon; Somerville, NJ), are then placed in a box pattern and tied tightly so as to create an unperfused area of upper uterine segment. Diathermy is used to open the uterus down to the membranes in the center of the “box” without blood loss ( Figure 2 and Video ). As shown in the Video , a finger is then inserted between the membranes and uterus to create a space into which 1 side of an 80-mm linear cutting stapler (DST Series GIA; Covidien, New Haven, CT) is introduced. The other side of the stapler is then attached and clamped closed, and the stapler is activated ( Figure 3 and Video ). Forward motion of the lever lays down 2 rows of staples, and backward movement of the lever divides the uterine muscle between the 2 staple lines. The stapler is removed, reloaded, and reintroduced 1 or 2 times as needed (taking care not to rupture the membranes) to create an avascular hysterotomy large enough to atraumatically deliver the baby ( Figure 4 ). The membranes are then opened and the baby is delivered.

A second way of introducing the stapler involves opening the exposed membranes and deploying the stapler inside the membranes. This carries the risk of including the cord or small parts of the fetus when clamping the stapler closed. Since there is no need to include the membranes in the staple line (as would be the case in a fetal surgery procedure) for safety reasons we prefer to deploy the stapler between the membranes and the wall of the uterus.
Following delivery of the baby the umbilical cord is clamped and cut without any attempt to remove the placenta, the clamped end of the cord is replaced in the uterine cavity, and the hysterotomy is closed with a running locked no. 1 polydioxanone suture (PDS-II) that incorporates the membrane edges ( Figure 5 ). The hysterectomy then proceeds. In most cases there is minimal blood loss (usually <20 mL) from the cesarean delivery. We have used this technique in 3 patients and noted <20 mL blood loss at the time of cesarean delivery in each case, with no need for transfusion during or after the cases. Case series involving ≤3 patients are exempt from institutional review board review at Baylor College of Medicine since interesting observations on this number of patients does not meet the definition of research as a systematic investigation designed to contribute to generalizable knowledge. The patients gave informed written consent to use their images/videos. The authors note that only those facile and experienced with the cutting stapler device should attempt its use for the purposes described in this article.