Microgastria and Gastric Perforation
Andrea Winthrop and Jill Whitehouse
MICROGASTRIA
Congenital microgastria is a rare anomaly that is characterized by failure of the primitive foregut to differentiate into a stomach during weeks 4 to 8 of gestation, thus resulting in a small tubular stomach usually associated with megaesophagus and incomplete gastric rotation (Fig. 400-1). Isolated microgastria is uncommon,1 with associated anomalies such as asplenia, situs inversus, limb hypoplasia, intestinal malrotation, laryngotracheal clefts, and cardiac abnormalities being common.2,3 Only about 60 cases have been described.
 CLINICAL MANAGEMENT AND OUTCOME
CLINICAL MANAGEMENT AND OUTCOME
Typically, patients present with recurrent vomiting, failure to thrive, and recurrent respiratory infections due to the reduced gastric volume and associated megaesophagus. Patients will often have persistent diarrhea due to dumping syndrome resulting from the lack of gastric capacity. Diagnosis of microgastria is by upper GI contrast studies that demonstrate the typical findings of a very small stomach. When identified, screening for associated anomalies is warranted.
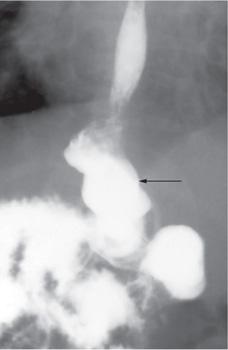
FIGURE 400-1. Upper GI radiograph showing the typical small-volume tubular stomach, incomplete rotation, and gastroesophageal reflux in a patient with microgastria.
The approach to management of microgastria is controversial. Case reports describe successes and failures of medical and surgical management approaches.4,5 Medical management was associated with poor growth, delay in cognitive development, and dumping syndrome, so that surgical therapy was recommended. However, improved technologies that allow routine use of gastric or jejunal slow-drip feedings has been reported to have successful outcomes.6 This approach prevents gastroesophageal reflux and allows appropriate nutrition for growth. Proton-pump inhibitor therapy may be beneficial since it can reduce gastric fluid volumes. Small oral feedings may be administered to allow appropriate development of feeding skills. Parenteral supplementation should not be required if jejunal feeding can be maintained. In children where drip feeds are tolerated gastric volume may increase significantly over the first years of life, and the patient can eventually be converted to bolus or ad lib feeds.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


