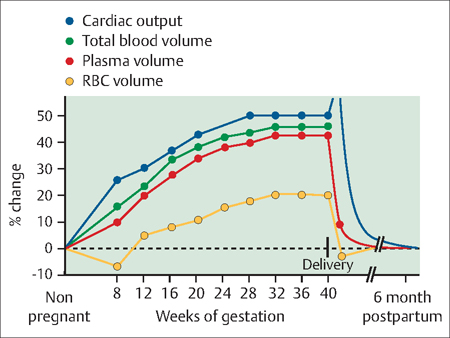
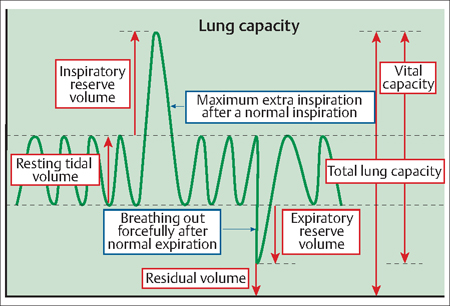
8 Maternal—Fetal Physiology Natalia P. Zef and Gustavo F. Leguizamón During pregnancy, extensive physiologic changes occur in both the mother and her developing fetus. Physiological activity increases markedly in most pregnant women, and an understanding of these normal physiological changes is necessary in order to provide adequate care. Furthermore, physicians caring for pregnant women must have a basic knowledge of embryology and fetoplacental physiology. Early pregnancy can be viewed as an anabolic state, with increased peripheral utilization of glucose and fasting hypoglycemia. Therefore, energy is stored in this early stage to meet future fetal demands in late pregnancy. The second half of pregnancy is characterized by a significant increase in insulin resistance and, consequently, postprandial hyperglycemia. Two common symptoms/findings presented by pregnant women can be explained by the following physiologic changes. Hyperglycemia also is associated with significant fetal complications. Since glucose readily crosses the placenta by facilitated diffusion, abnormal values in the maternal compartment are immediately followed by abnormal fetal glycemic levels. Therefore achieving euglycemia during pregnancy is of utmost importance (see Evidence Box 8.1). Pregnancy affects all of the components of the mother’s cardiovascular system, including cardiac volume and output as well as blood volume and red blood cell count (Fig. 8.1). Changes in cardiac function begin in the first trimester of pregnancy. There is an initial increase in cardiac output due to reduced systemic vascular resistance, and an increase in heart rate, which continues to increase and remains elevated during the remainder of pregnancy. At just about mid-pregnancy, arterial blood pressure decreases to a nadir and rises thereafter until term, but even then, it is still 21% lower than nonpregnant values. This overall decrease in maternal blood pressure is a result of the decreased systemic vascular resistance due to the smooth muscle-relaxing effects of the elevated progesterone levels. Fig. 8.1 Beginning in the first trimester, many changes occur in a pregnant woman’s cardiovascular and hematologic system to compensate for the need to supply additional blood and nutrients to her growing body and the fetus The diaphragm rises by about 4 cm during pregnancy, causing a reduction in the lung residual volume. The increased ventilation observed during pregnancy is secondary to increased tidal volume (TV) with no change in the respiratory rate (RR). This is caused by a direct effect of progesterone on the CNS respiratory center. Functional residual capacity (FRC) is defined as the volume remaining in the lungs after a forced expiration. The increase in TV observed occurs at expense of the FRC. The VC does not change (Fig. 8.2). Minute ventilation is defined as tidal volume (TV) x respiratory rate (RR). The increase observed in minute ventilation is responsible for the physiologic fall of the Paco 2 and the Paco2. This fall facilitates the transfer of CO2 from the fetus to the mother and results in respiratory alkalosis observed under physiological conditions in pregnancy. Spirometric measurements and peak expiratory flow rates are not altered in pregnancy, suggesting that airway function remains stable. However, despite pulmonary function not being altered during pregnancy, diseases of the respiratory tract may be more serious. Indeed, pregnancy increases the woman’s risk of a number of non-infectious respiratory diseases, including asthma, aspiration pneumonia, venous air embolism, adult respiratory distress syndrome, pulmonary embolism, and deep venous thrombosis. These conditions often have unique manifestations in pregnant women. Fig. 8.2 Lung capacity is the total volume of the lung (i e, the volume of air in the lungs after maximum inspiration) It is calculated by adding the inspiratory reserve volume to the tidal volume plus expiratory reserve volume and the residual volume (IRV + TV + ERV + RV) The increase in oxygen requirement caused by pregnancy is accommodated by an increase in tidal volume without an increase in respiratory rate During pregnancy, the kidneys enlarge significantly, owing to an increase in their vasculature, interstitial volume, and urinary dead space (, dilation of the renal pelvis, calyces, and ureters) and reach their maximal size by mid-pregnancy.
Maternal Physiology
Carbohydrate Metabolism
Cardiovascular System
Respiratory Tract
Renal function
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


