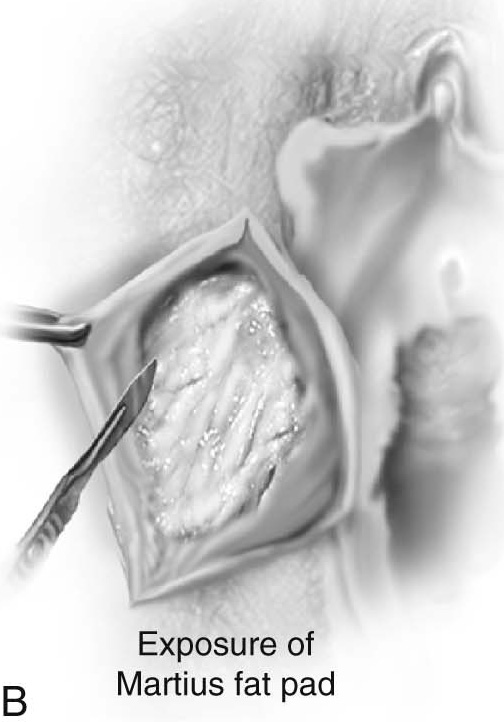
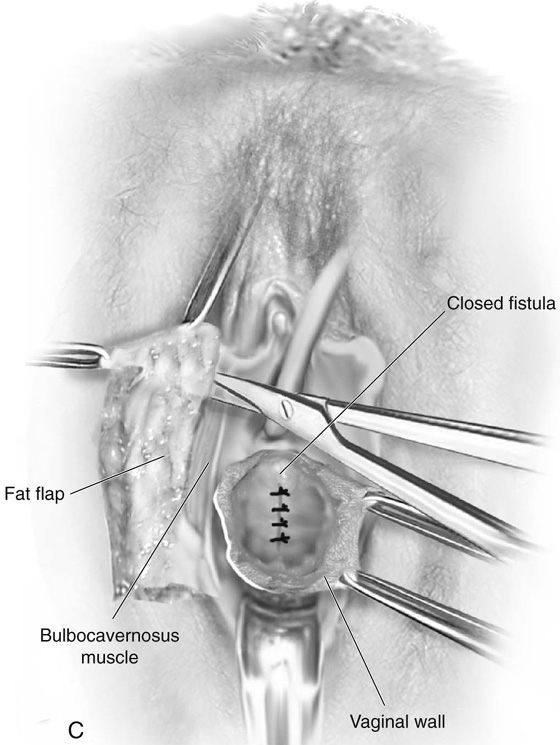
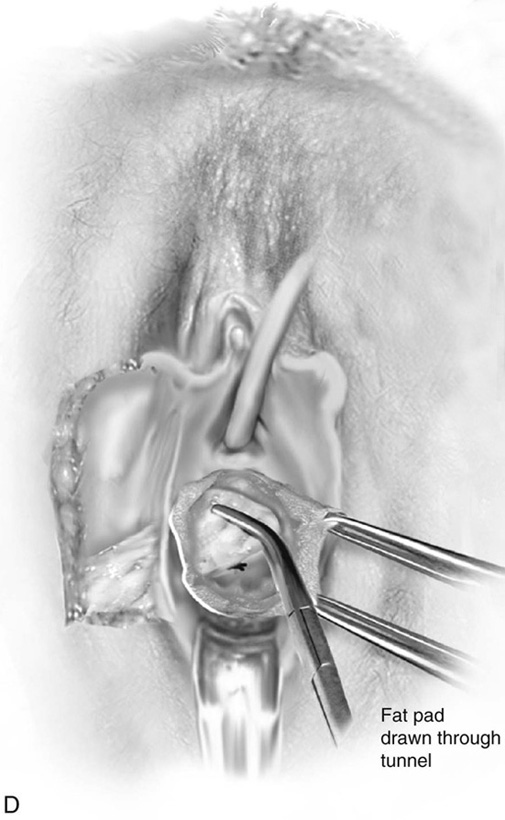
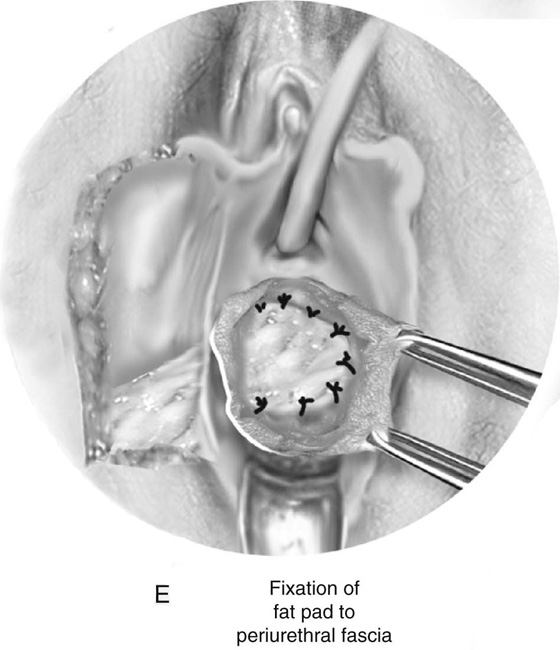
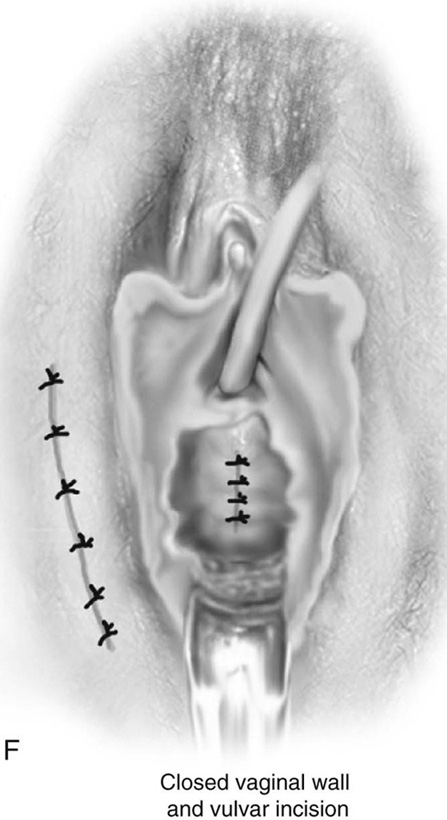
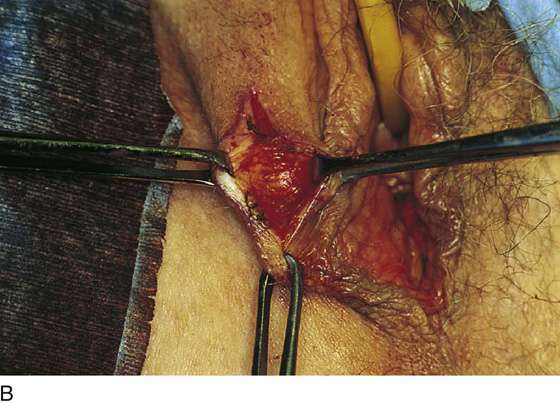
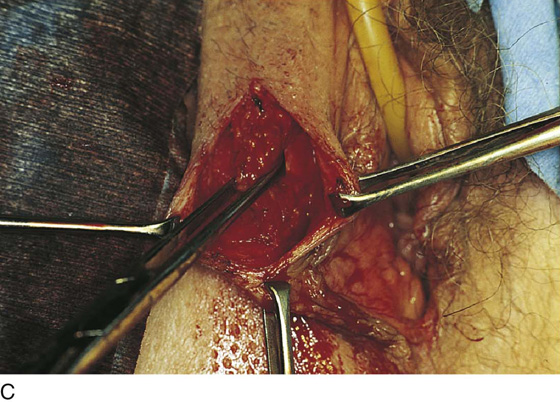
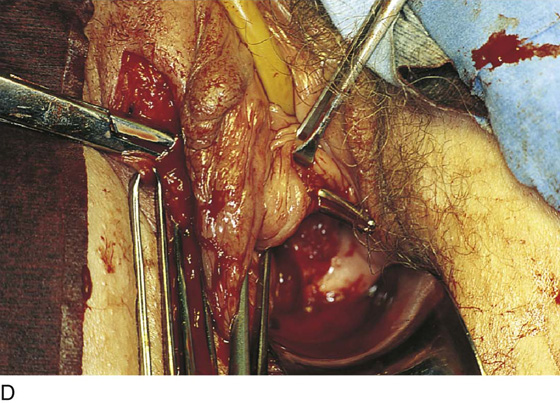
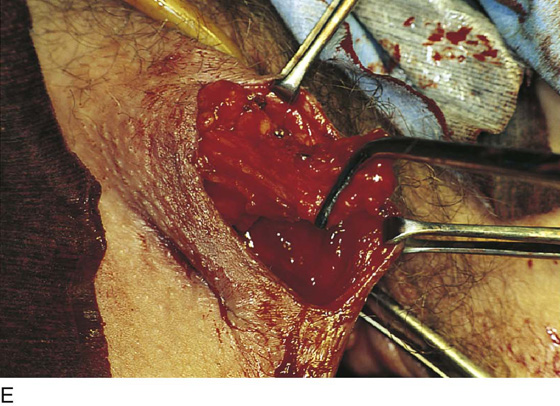
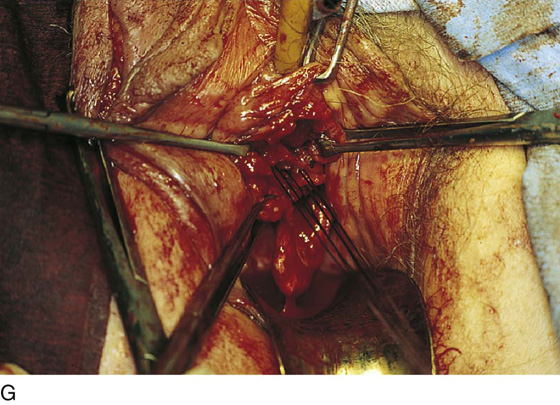
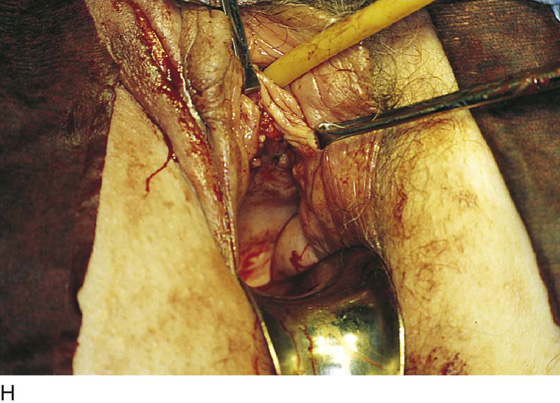
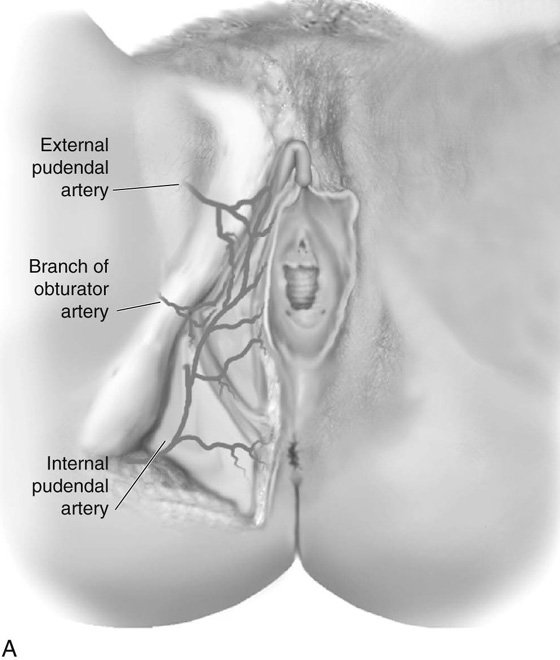
CHAPTER 85 Transposition of a labial fat pad with or without the bulbocavernosus muscle has been used to facilitate closures of fistulas involving the anterior and posterior vaginal wall. The procedure yields tissues that can fill in dead space and provide an excellent blood supply. The fact that this operation does not alter the anatomy of the vulva and is cosmetically pleasing is also important. Fig. 85–1A demonstrates the abundant blood supply to the labial fat. It has been empirically stated that the majority of the blood supply comes from the inferior direction (internal pudendal artery); thus the detachment of the fat should be anterior. Our dissections and experience with the procedure would indicate that sufficient blood supply is present from both directions; thus detachment should be at the discretion of the surgeon and more related to the anatomic location of the defect in the vagina. The procedure begins by marking an incision over the labial fat. The fat pad is mobilized on each side. After the vaginal dissection has been completed, a long curved clamp is passed medially into the vaginal incision, thus creating a tunnel that the fat pad will pass through to reach the vaginal area. The fat pad is then detached either anteriorly or posteriorly and passed into the vaginal area and fixed with delayed absorbable sutures. The vaginal and labial incisions are closed without tension (see Figs. 85–1 and 85–2). FIGURE 85–1 Technique of Martius fat pad transposition. A. Blood supply to the labial fat. B. Exposure of the fat pad via labial incision. C. Mobilization of fat. D. Anterior detachment of the fat pad with tunneling into the vaginal incision and fixation of the fat pad over the closed urethrovaginal fistula. F. Closure of the vaginal and labial incisions. FIGURE 85–2 Technique of labial fat pad transposition. A.
Martius Fat Pad Transposition and Urethral Reconstruction
Martius Fat Pad Transposition

![]()
Stay updated, free articles. Join our Telegram channel


Full access? Get Clinical Tree


