Management of Laryngotracheal Obstruction in Children
Pediatric surgeons are often involved in the management of acute and chronic airway obstruction. Moreover, iatrogenic injury to the pediatric airway occasionally occurs. The large number of operative techniques for the treatment of laryngotracheal stenosis shows that no single procedure or technique is universally applicable and successful. Prevention of, or prompt therapy for, injury is all important.1,2
Practical Embryology and Anatomy
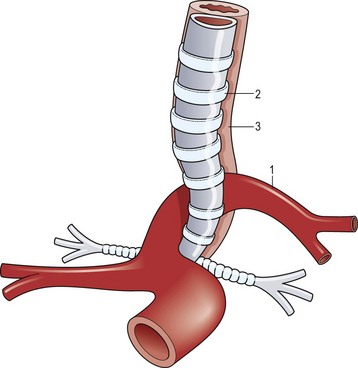
A working knowledge of the embryonic development of the mediastinal structures aids in understanding the etiology and associated anomalies of tracheal obstruction. Malformations of the great vessels (vascular rings) should be suspected and investigated when evaluating a child with complete tracheal rings. The most common vascular malformation associated with complete tracheal rings is a pulmonary vascular sling. This anomaly occurs when the left pulmonary artery arises to the right of the trachea, around which it curves and compresses just above the carina, and then passes between the trachea and esophagus before reaching the left lung (Fig. 21-1).3 Other vascular ring malformations may produce varying degrees of tracheal, bronchial, and esophageal compression.
Subglottic and Tracheal Malformations
Congenital Subglottic and Tracheal Stenosis
The anatomy of the pediatric airway has been compared to an inverted cone, with the trachea fitting telescopically into the cricoid above it, the cricoid into the thyroid cartilage, and then the thyroid into the hyoid space (Fig. 21-2).4 Congenital subglottic stenosis is the most common morphologic abnormality and presents as a narrowing of the airway at the distal end of the larynx, just at the beginning of the trachea. The subglottic region lies at the level of the cricoid cartilage, which is normally the only complete cartilaginous ring in the airway. Congenital subglottic abnormalities result in elliptical narrowing of the cricoid cartilage, the etiology of which is not known. Subglottic stenosis is exceeded only by laryngomalacia and vocal cord paralysis in the frequency of congenital airway anomalies.
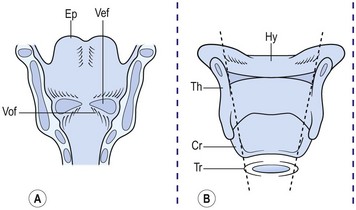
FIGURE 21-2 (A) Ventral area of the larynx in the neonate viewed from behind. The ventricle, or ‘third cavity,’ is bounded above by the ventricular folds (Vef) and below by the vocal folds (Vof). Ep, epiglottis. (B) Laryngeal cartilages (without arytenoids). Th, thyroid; Cr, cricoid; Tr, trachea; and Hy, hyoid viewed from behind. Inner dashed lines show telescopic configuration in the neonate as opposed to the rectangular shape in the adult (outer dashed lines). (Adapted from Othersen HB Jr, editor. The Pediatric Airway. Philadelphia: WB Saunders; 1991.)
When compared with an adult, the anatomy of the trachea and larynx of a child differs in several ways (Fig. 21-3). The child’s epiglottis is short and small, and the valleculae are shallow. Also, the larynx points posteriorly, and the arytenoid apparatus is large in relation to the lumen of the larynx. Finally, the narrowest point of the normal pediatric airway is the subglottis. In the adult, it is the glottis.
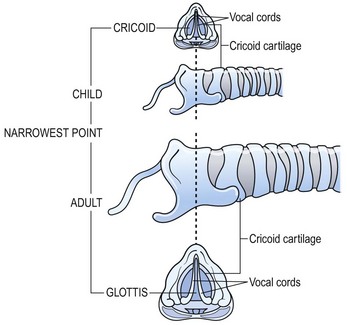
FIGURE 21-3 Difference between adult and pediatric airway. (Adapted from Othersen HB Jr. Intubation injuries of the trachea in children: Management and prevention. Ann Surg 1978;189:601–6.)
Acquired Subglottic and Tracheal Stenosis
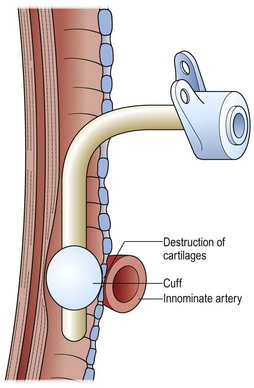
Acquired airway malformations usually result from intrinsic injury with subsequent inflammation, ulceration, and scarring, leading to subglottic or tracheal scarring and narrowing. Occasionally, trauma is the initiating event but an iatrogenic event can exacerbate an unstable situation.2 For example, a child with a congenitally small airway might be asymptomatic until an endotracheal tube is inserted. The tube may be appropriate in size but, because of the congenital stenosis, it will fit tightly and can lead to ulceration and stricture. Particularly difficult to treat are those injuries that occur well below the subglottic region, usually produced by an endotracheal balloon that caused compression and ulceration in the trachea. Frequently, these areas of injury are below the usual site for a tracheostomy. The cuff may even erode into overlying vessels (Fig. 21-4).
Vascular Compression
Compression and partial obstruction of the trachea may be caused by abnormalities of the aortic arch that impinge on, or encircle, the trachea or esophagus, or both.5,6 When both the trachea and esophagus are compressed, swallowing frequently produces airway compression and respiratory distress. Vascular rings are often asymptomatic in neonates and infants, yet can lead to significant airway obstruction in a child.7
The physiologic impingement on the trachea by a vascular ring is similar to that seen in patients after repair of esophageal atresia. The persistently distended upper esophageal pouch can displace the trachea anteriorly, producing tracheomalacia (Fig. 21-5). Particularly with swallowing, the distended esophageal pouch may compress the trachea against the innominate artery (Figs 21-6 and 21-7). Correction of this problem centers on anterior mobilization and suspension of the innominate artery (Fig. 21-8).8–12 The treatment of a pulmonary vascular sling may require not only relocation and reimplantation of the pulmonary artery, but also repair of the stenotic distal trachea.7,12,13
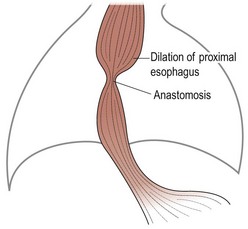
FIGURE 21-5 After repair of esophageal atresia, the proximal esophagus, which is already enlarged, is further dilated by an anastomotic stricture. (Adapted from Othersen HB Jr, editor. The Pediatric Airway. Philadelphia: WB Saunders; 1991.)
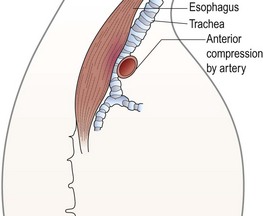
FIGURE 21-6 A lateral view shows how the dilated proximal esophagus displaces the trachea and compresses it against the overlying innominate artery. (Adapted from Othersen HB Jr, editor. The Pediatric Airway. Philadelphia: WB Saunders; 1991.)
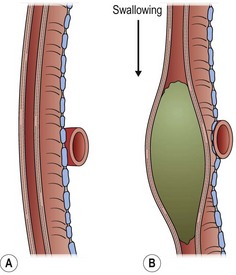
FIGURE 21-7 An enlarged diagram of Figure 21-6 illustrates how the compression is increased by ingestion of food. (Adapted from Othersen HB Jr, editor. The Pediatric Airway. Philadelphia: WB Saunders; 1991.)
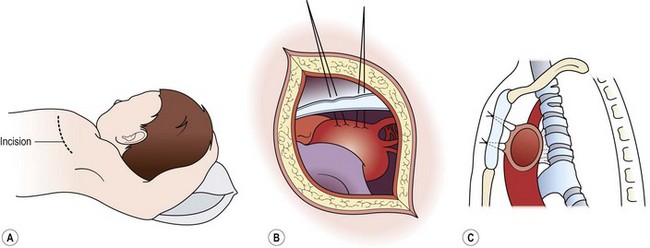
FIGURE 21-8 The operative technique for aortopexy. (A) Anterior left thoracotomy in the third interspace. (B) Sutures placed into the wall of the innominate artery and the aortic arch. (C) Sutures passed through the sternum and tied to elevate the compressing vessels. Tracheal attachments pull the anterior wall of the trachea forward. (Adapted from Othersen HB Jr, editor. The Pediatric Airway. Philadelphia: WB Saunders; 1991.)
Stridor and dyspnea are symptoms that can be produced by vascular impingement on the trachea. Patients with severe compromise from a double aortic arch are usually symptomatic, but their manifestations are variable (Fig. 21-9). Some patients are seen with frequent coughing episodes and stridor accompanied by dyspnea and cyanosis, whereas small infants may have apneic episodes. The symptoms of vascular impingement on the trachea are usually more dramatic than those from compression of the esophagus.
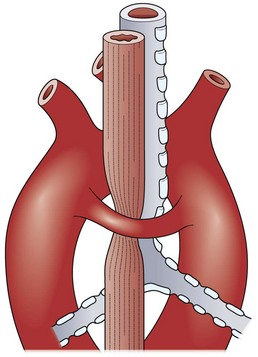
FIGURE 21-9 Both trachea and esophagus are compressed by a double aortic arch. (Adapted from Othersen HB Jr, editor. The Pediatric Airway. Philadelphia: WB Saunders; 1991.)
Classically, vascular ring anomalies are diagnosed on a barium esophagogram with indentations on the esophageal column of barium and a decrease in the tracheal air column. Offset of the axis of the barium column above and below the indentation is diagnostic of a double aortic arch (Fig. 21-10A). More recently, rapid computed tomographic (CT) scans allow a graphic reconstruction of the trachea and adjacent vessels (Fig. 21-10B). Magnetic resonance imaging (MRI) enhanced with intravenous administration of a contrast agent allows excellent visualization of the trachea and vessels as well.
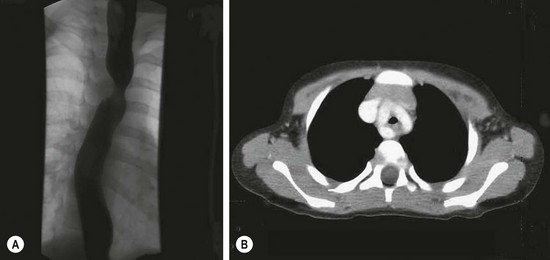
FIGURE 21-10 This infant presented with stridor. There was a suggestion of tracheal indentation on the chest radiograph. Therefore, a barium esophagogram was performed (A) and shows the double indentations diagnostic of a double aortic arch. (B) A CT scan shows contrast in the double arch that is encircling the trachea and esophagus (collapsed).
Occasionally, a child will appear with acute airway obstruction or other medical problems requiring intensive care, during which endotracheal intubation and a concomitant nasogastric tube are inserted. The presence of tubes in both airway and esophagus makes detection of a vascular ring difficult and can generate complications. In a child who is already intubated, performance of contrast radiographic procedures may not be possible. Ultrasonography (US), or CT, or contrast-enhanced MRI may delineate the vascular abnormality. When both tracheal and esophageal intubations are necessary in a patient with a double aortic arch, the encircling vessels may sustain pressure necrosis. Erosion into the aortic arch can produce an aortoesophageal fistula that may not be manifest until either the endotracheal or the esophageal tube is removed. A sentinel hemorrhage may occur before a massive, and often fatal, hemorrhage occurs into the esophagus. The passage of a Sengstaken–Blakemore tube with inflation of the esophageal balloon can be life-saving by tamponading the fistula.14 Because no reliable diagnostic study is available to demonstrate an aortoesophageal fistula, the observation of a sentinel hemorrhage in such a patient with ultrasound confirmation of a double aortic arch is a clear indication for urgent cardiopulmonary bypass and repair.14
Vascular rings cause airway constriction and not vascular problems. Thus, simple division of the vascular ring is often not enough to relieve tracheal compression. Following division of a vascular ring, if part of the ring continues to compress the airway, it should not be dissected away from the trachea but suspended anteriorly, often to the back of the sternum. The vascular-tracheal attachments will lift the anterior tracheal wall and enlarge the lumen (see Fig. 21-8). Traditionally, an open operation has been used for vascular ring repair. Significant numbers of patients are now being treated by the thoracoscopic approach.15 Regardless of the approach, whether from the right or from the left,16 or other technical variations,17 the recurrent laryngeal and phrenic nerves need to be identified and protected. Flexible endoscopic observation of the trachea during these maneuvers can corroborate relief of the compression.6
Tracheomalacia
Often, tracheomalacia is produced by constant pressure from a cardiovascular structure. Thus it is almost always necessary to suspend the offending vessel and utilize its attachments to the trachea to expand the tracheal lumen. Tracheomalacia can be primary in nature without evidence of compression. In these cases, suspension of the large mediastinal vessels may enlarge the tracheal lumen, or the peritracheal fascia can be suspended to the sternum to overcome collapse of the airway.18–21 In the UK (Scotland), guidelines have been promulgated for the use of thoracoscopic aortopexy to treat severe primary tracheomalacia. Interestingly, the National Health Service believed that these guidelines were necessary because individual surgeons would operate infrequently on infants and children who are good candidates for operative correction.
Inflammatory Obstructions
Viral laryngotracheitis (croup), bacterial or membranous tracheitis, and epiglottitis are inflammatory conditions that occasionally require operative intervention. In cases of inflammatory obstruction, endotracheal intubation is preferred instead of tracheostomy if possible. It is important to distinguish croup and bacterial tracheitis from epiglottitis because the treatments are quite different (Table 21-1).
TABLE 21-1
Characteristics of Laryngotracheobronchitis and Epiglottitis
| Characteristic | Laryngotracheobronchitis | Epiglottitis |
| Incidence | Common | Uncommon |
| Etiology | Viral | Haemophilus influenzae type b |



