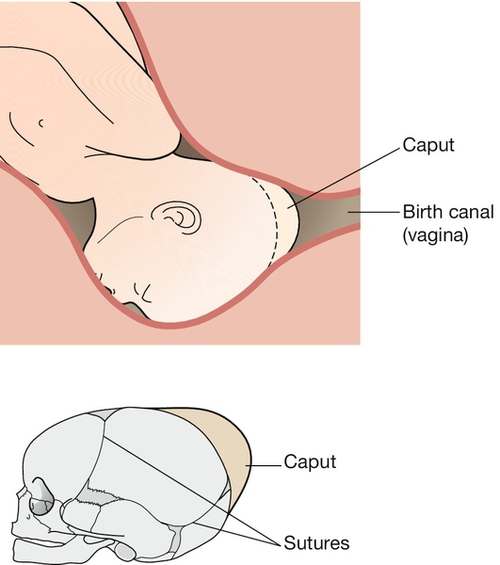
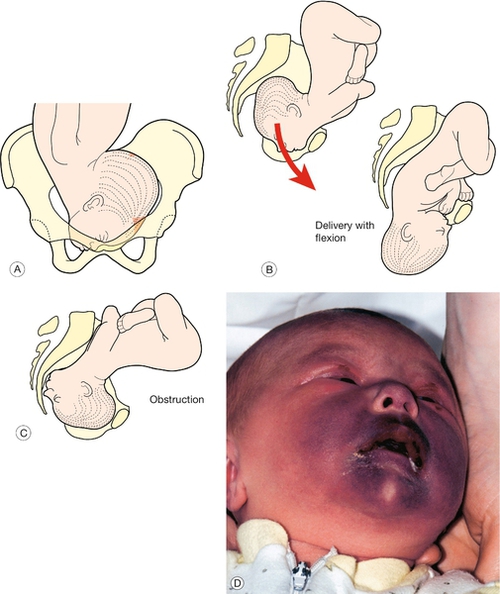
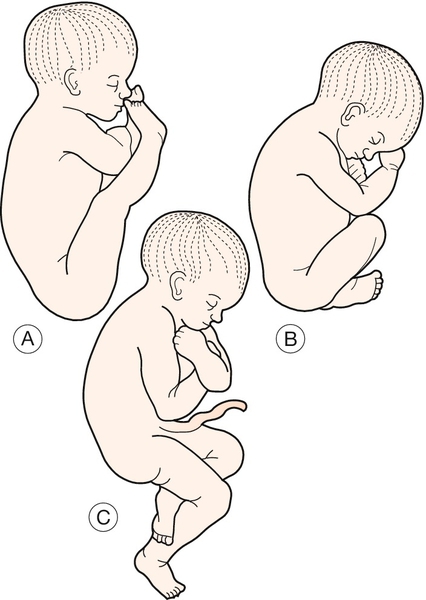
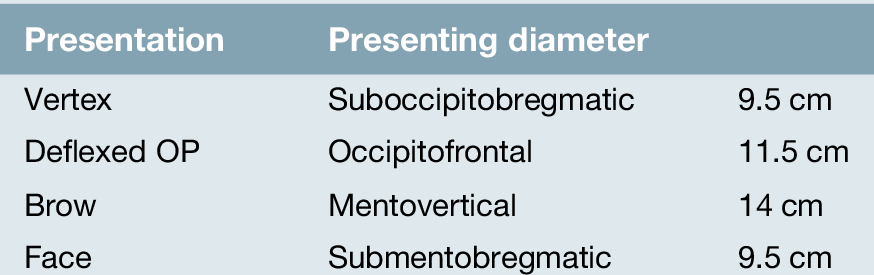
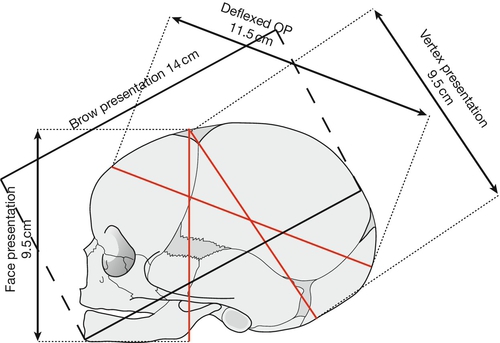
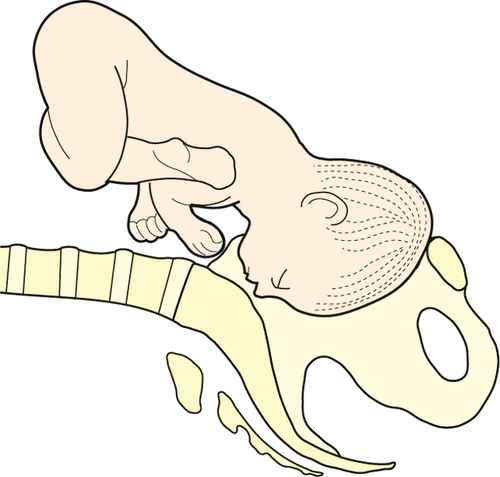
45 During pregnancy, abdominal palpation should aim to define the lie, presentation and position of the fetus. The lie refers to the long axis of the fetus in relation to the long axis of the uterus. Usually, the fetus is longitudinal, but occasionally it may be transverse or oblique. The presentation is that part of the fetus which is at the pelvic brim, in other words the part of the fetus presenting to the pelvic inlet. Normal presentation is the vertex of the fetal head and the word ‘malpresentation’ describes any non-vertex presentation. This may be of the face, brow, breech, or some other part of the body if the lie is oblique or transverse. The position of the fetus refers to the way in which the presenting part is positioned in relation to the maternal pelvis. Strictly speaking this refers to any presenting part, but here it will be considered in relation to those fetuses presenting head first (cephalic). As we have seen, the head is usually occipitotransverse at the pelvic brim and rotates to occipitoanterior at the pelvic floor. ‘Malposition’ is when the head, coming vertex first, does not rotate to occipitoanterior, presenting instead as persistent occipitotransverse or occipitoposterior. As described above, ‘malpresentation’ is a term used to describe any non-vertex presentation. Over 95% of fetuses are in cephalic presentation at term. Malpresentations include face presentation, brow presentation and breech presentation. When the fetus has a cephalic presentation, the presenting diameter is dependent on the degree of flexion or extension of the fetal head – deflexed and brow presentations offer a wide diameter to the pelvic inlet (Table 45.1 and Fig. 45.1). As the fetal skull is made up of individual bony plates (the occipital, sphenoid, temporal and ethmoid bones), which are joined by cartilaginous sutures (the frontal, sagittal, lambdoid and coronal sutures), it has the potential to be ‘moulded’ during labour. This allows the head to fit the birth canal more closely (Fig. 45.2). Moulding should be distinguished from caput succedaneum, which refers to oedema of the presenting part of the scalp. Both moulding and caput can occur in any cephalic presentation, but are more likely to occur in malpresentation. The presence or absence of moulding and caput should be documented during each vaginal examination in labour; excessive moulding and caput are suggestive of an obstructed labour due to cephalopelvic disproportion. Caput refers to oedema of the presenting part of the scalp. This occurs in about 1:500 births and occurs when the fetal head extends right back (hyperextended so that the occiput touches the fetal back) (Fig. 45.3 A). It is associated with prematurity, tumours of the fetal neck, loops of cord around the fetal neck, fetal macrosomia and anencephaly. Face presentation is usually only recognized after the onset of labour and, if the face is swollen (Fig. 45.3 B), it is easy to confuse this presentation with that of a breech. The position of the face is described with reference to the chin, using the prefix ‘mento’. The presenting diameter is submentobregmatic (9.5 cm) (Fig. 45.1). (A) The head enters the pelvic brim in the transverse position. (B) Most rotate to the mentoanterior position and deliver without problems. (C) Those that rotate to mentoposterior will obstruct. (D) Face presentation is often associated with oedema and bruising. This baby recovered without problems. The face usually enters the pelvis with the chin in the transverse position (mentotransverse) and 90% rotate to mentoanterior so that the head is born with flexion (Fig. 45.3 C). If mentoposterior, the extending head presents an increasingly wider diameter to the pelvis, leading to worsening relative cephalopelvic disproportion and impacted obstruction (Fig. 45.3 D). A caesarean section is usually required. This occurs in only approximately 1:700 and 1:1500 births and is the least favourable for delivery (Fig. 45.4). The presenting diameter is mentovertical, measuring 14 cm. The supraorbital ridges and the bridge of the nose will be palpable on vaginal examination. The head may flex to become a vertex presentation or extend to a face presentation in early labour. If the brow presentation persists, a caesarean section will be required. Breech presentation describes a fetus presenting bottom first. The incidence is around 40% at 20 weeks, 25% at 32 weeks and only 3–4% at term. The chance of a breech presentation turning spontaneously after 38 weeks is < 4%. Breech presentation is associated with multiple pregnancy, bicornuate uterus, fibroids, placenta praevia, polyhydramnios and oligohydramnios. It may also rarely be associated with fetal anomaly, particularly neural tube defects, neuromuscular disorders and autosomal trisomies. At term, 65% of breech presentations are frank (extended) with the remainder being flexed or footling (Fig. 45.5). Footling breech carries a 5–20% risk of cord prolapse (p. 367). Those presenting by the breech may be (A) extended (or frank); (B) flexed; or (C) footling.
Malpresentations and malpositions
Introduction
Malpresentation
Face presentation
Brow presentation
Breech presentation
Mode of delivery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


