for invasive cancer may be greater with perianal location, increased age, immunosuppression, and previous radiotherapy.
 FIGURE 49.1 Invasive squamous cell carcinoma of the vulva. This is a 1.8-cm ulcerative lesion on the right anterior vulva. |
 FIGURE 49.2 Carcinoma in situ of the vulva. Vulvar intraepithelial lesions can be white, brown, or red. |
 FIGURE 49.3 Invasive carcinoma of the left vulva with extensive associated carcinoma in situ involving both labia. |
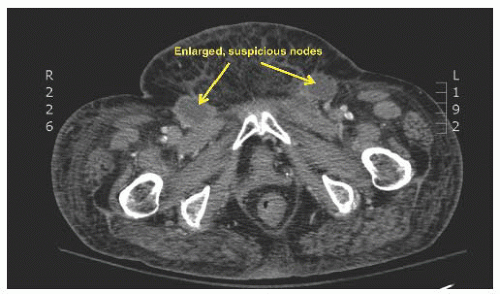 FIGURE 49.4 Computerized tomography (CT) image of the inguinal area showing enlarged lymph nodes typical for metastatic cancer (arrows). |
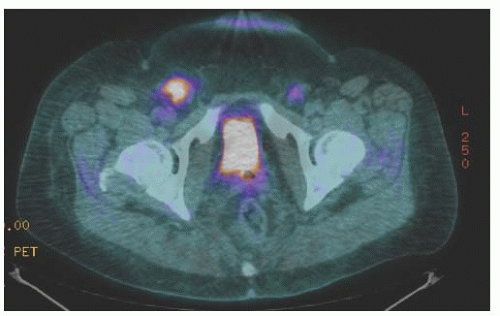 FIGURE 49.5 Positron emission tomography (PET) of the groin areas showing significantly increased FGD uptake in bilateral nodes very typical of metastatic cancer (same patient as in Fig. 49.4). |
TABLE 49.1 2009 FIGO Staging System for Vulvar Cancer | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
TABLE 49.2 Tumors with Invasion of Less Than 1 mm with Nodal Disease, Either at Diagnosis or Recurrence | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
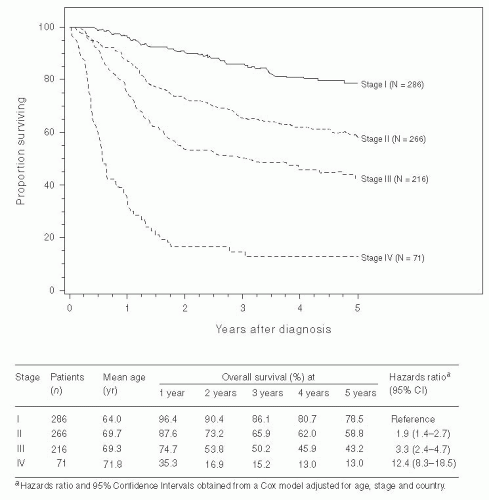 FIGURE 49.6 Survival curves for patients with squamous cell carcinoma of the vulva related to FIGO stage. These patients were treated from 1999 through 2001 and were staged according to the FIGO staging system of 1996. (Reprinted from Beller U, Benedet JL, Creasman WT, et al. Carcinoma of the vagina: 26th Annual report on the results of treatment in gynecological cancer. Int J Gynecol Obstet 2006;95:S29-S42, with permission. Copyright © 2006 International Federation of Gynecology and Obstetrics. Published by Elsevier Ireland Ltd. All rights reserved.) |
nodes or with bilateral nodal involvement. On the basis of limited data from a few studies, it appears that large nodal diameter, extensive nodal replacement, and especially extracapsular extension of a lymph node metastasis are adverse prognostic factors. In a report by Origoni and colleagues in 1992 that was based on 53 vulvar cancer patients with groin node metastases, the survival rate varied from 90.9% when the diameter of the metastasis was less than 5 mm to 20% when it was larger than 15 mm, and from 85.7% to 25% when the metastases were intracapsular and extracapsular, respectively. Especially important are the data from the 19 patients in that study with a single positive node. For these patients, the 5-year cancerrelated survival rate was 90% when the metastasis diameter was less than 5 mm versus 37.5% when it was 15 mm, and 85.7% when the metastasis was intracapsular versus 20% when it was extracapsular. Results from a study by Paladini and associates were similar; they reported that patients with intracapsular metastases tended to have recurrence at distant sites, whereas patients with extracapsular nodal disease were more likely to have local or groin recurrence.
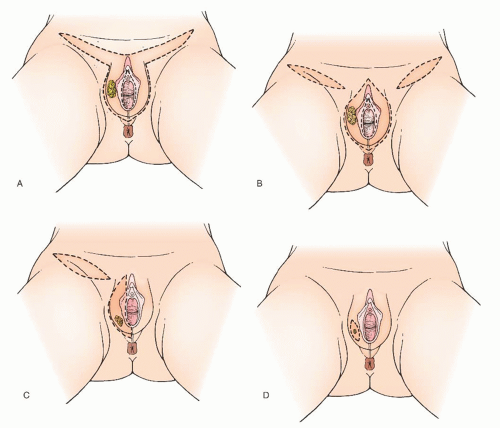 FIGURE 49.7 Modification in regional lymph node management. A: En bloc removal. B: Radical vulvectomy with bilateral inguinal-femoral lymphadenectomy through three separate incisions. C: Unilateral lymphadenectomy for a well-lateralized lesion. D: Early lesion with omission of lymphadenectomy. |
to the en bloc radical resection include urinary or fecal incontinence and vaginal prolapse. The “one-size-fits-all” approach of treating all patients with the same radical vulvectomy and inguinal-femoral lymphadenectomy resulted in overtreatment of many patients and undertreatment of some with inadequate attention to local margin and the risk of lymph node metastasis. The following section provides a more individualized approach based on current literature and extensive surgical experience.
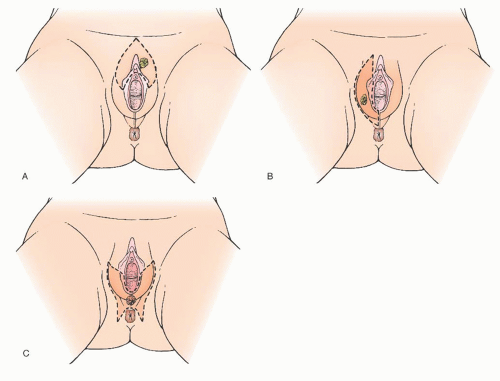 FIGURE 49.8 Modified radical vulvectomy. A: Anterior hemivulvectomy. B: Right hemivulvectomy with clitoral sparing. C: Posterior hemivulvectomy. |
years, the extent of the radical vulvectomy has been modified to emphasize wide excision of the primary cancer with adequate skin and deep margins but not necessarily radically resecting the entire (uninvolved) vulva. Recommendations have included 1- to 3-cm skin margins for well-localized, unifocal lesions and to the depth of the inferior fascia of the urogenital diaphragm. The main type of morbidity relating to increasing the radicality of vulvectomy is subsequent sexual dysfunction and disfigurement. Modification of the surgical resection or the use of neoadjuvant chemoradiation should be considered to avoid compromising the function of the anus or urethra. In a 1979 study, DiSaia and colleagues reported complete preservation of sexual function in 17 of 18 patients who underwent wide local excision for early invasive tumors. They also reported that preservation of the mons pubis as well as the major portion of the superior aspect of the vulva resulted in an appreciably more satisfactory cosmetic result.
TABLE 49.3 Modified Radical Vulvectomy Literature: Local Recurrence | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
good results with the use of cutaneous rhomboid flaps in the reconstruction of the perineum and perianal area. These flaps allow for reconstruction of a perineal body, they bring tissue with a good blood supply into the area that promotes healing, and they allow closure of the wound without tension on the anus. However, if there is concern that these functional structures would be sacrificed in order to obtain margins, strong consideration should be given to neoadjuvant treatment as discussed later in the chapter.
 FIGURE 49.9 Invasive squamous cell carcinoma involving the perineum and perianal skin. Note the pigmented lesions of carcinoma in situ adjacent to the ulcerated invasive cancer. |
and ipsilateral superficial inguinal lymphadenectomy were performed, and 121 patients were evaluable. These were compared with a historical control group in the GOG registry who had undergone radical vulvectomy with bilateral inguinofemoral lymphadenectomy. Nine patients in this study, or 7.3%, experienced groin recurrences versus no recurrence in the control group. Six of the groin recurrences were in the ipsilateral groin, and 5 of the 9 patients died of the recurrent vulvar cancer. The interpretation from this study was that superficial inguinal lymphadenectomy may not be adequate treatment even for early vulvar carcinoma. However, in a number of patients in this study, the tumors approached the midline; there is evidence that more medial tumors may have direct drainage to the deep inguinal lymph nodes. Another area of concern in this study is the high percentage of poorly differentiated tumors—almost twice as many as in the control group. Six of the nine groin recurrences in this study were from the poorly differentiated tumors. Whether poorly differentiated tumors are more likely to metastasize to deep inguinal or contralateral inguinal lymph nodes deserves further study. Subsequent additional retrospective data from large cancer centers also report a 5% to 10% incidence of groin relapse in patients with negative nodes from superficial inguinal lymphadenectomy.
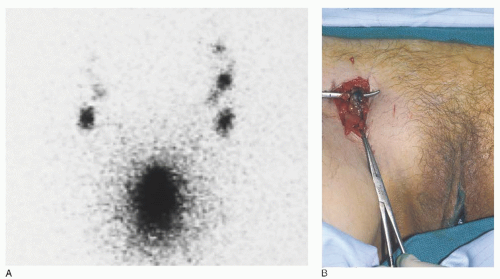 FIGURE 49.10 A: Preoperative lymphoscintigram 60 minutes after intralesional injection of technetium-99. B: Intraoperative blue node blue sentinel node in the right groin after injection of isosulfan blue dye into the primary vulvar cancer. |
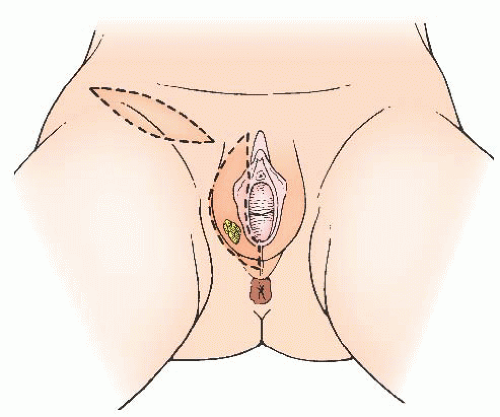 FIGURE 49.11 Unilateral lymphadenectomy in a patient with a focal right-sided small vulvar primary. |
risk of contralateral nodal metastases. Patients with tumors approaching the midline or involving more medial structures (perineum, clitoral hood or clitoris, vagina, and labia minora) are at increased risk for contralateral lymph node metastases. The issue of unilateral groin lymphadenectomy was studied to some extent in 1992 by Stehman and associates in a GOG study. Patients with early disease and negative ipsilateral superficial inguinal lymph nodes were treated with ipsilateral superficial inguinal lymphadenectomy and a modified radical vulvectomy. A few patients in this study did have a bilateral inguinal lymphadenectomy because of midline involvement. A total of 121 patients were in the study, and 3 experienced contralateral inguinal lymph node recurrences. The vulvar lesions of these 3 patients ranged from 0.6 to 2.5 mm in depth of invasion, and all were poorly differentiated. Although lesion location was not given for these 3 cases, a large percentage of patients included in this study had lesions approaching the midline, as defined by involvement of the labia minora. Tumors with capillary or lymphatic space involvement were excluded from this study.
 FIGURE 49.12 Classic en bloc resection of the vulva and inguinal-femoral nodes through one interconnected incision. |
incisions are used, and the same vulvar tissue is excised (Fig. 49.13A). The superior incision extends from the top of the labiocrural folds as an inverted V, with the point above the base of the clitoris. As previously discussed, a variable amount of superior tissue (i.e., mons pubis) is removed, depending on the location and size of the lesion.
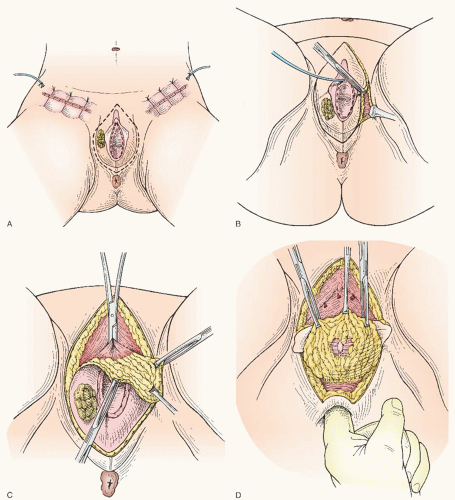 FIGURE 49.13 Radical vulvectomy with bilateral inguinal lymphadenectomy done through three separate incisions. A: Bilateral inguinofemoral lymphadenectomy through separate incisions is completed. Separate incision for radical vulvectomy is marked. B: Labiocrural incisions are extended to deep fascia of the urogenital diaphragm. C: Dissection proceeds dorsally off of the pubic bone. The vascular base of the clitoris is clamped, followed by transection and ligation. D: Perineal body and posterior vulvar tissues are dissected away from the anus. |
anus, or distal urethra. For an anterior lesion, it is reasonable to spare the perineal body; but for a posterior lesion, it is important to incorporate radical resection of this area. For a lesion (especially superficial) in proximity to the urethral meatus or anus, it is reasonable to limit the margin of resection to 1 cm (but not less) to preserve these structures and their function.
 FIGURE 49.13 (Continued) E: The vascular vestibular tissue along the sides of the vaginal tube is clamped. Transection and suture ligation to follow. F: Radical vulvectomy resection is completed. G: Closure of the vulvar wound is completed. |
underlying deep fascia of the urogenital diaphragm is completed. Clamps and transfixion suture ligatures of no. 0 or 2-0 polyglactin are used during transection of the tissue along the side of the vaginal tube in the region of the vestibular bulbs (Fig. 49.13E).
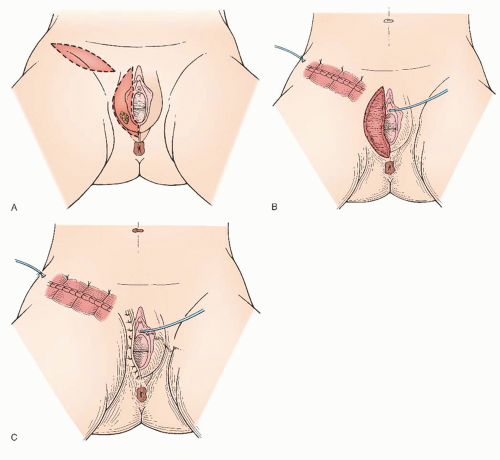 FIGURE 49.14 Modified right radical vulvectomy and unilateral right inguinal-femoral lymphadenectomy. |
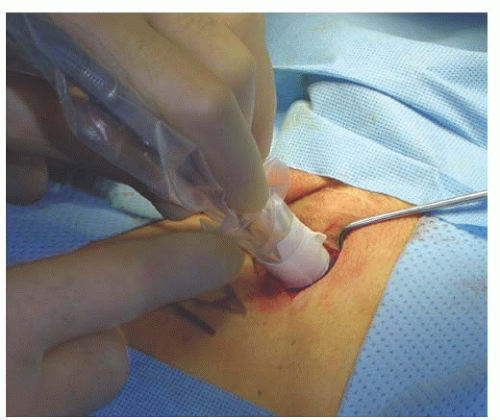 FIGURE 49.15 Intraoperative use of the gamma probe to identify the radioactive sentinel node. |
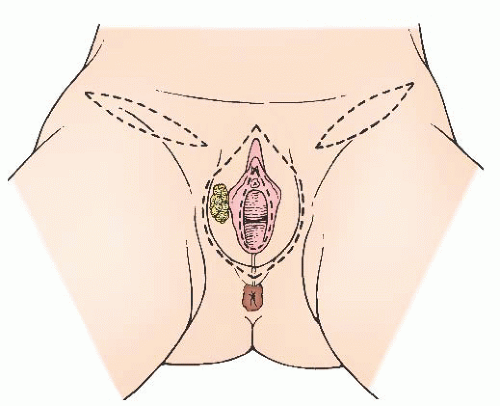 FIGURE 49.16 Separate incisions for bilateral lymphadenectomy done with a radical vulvectomy. |
lymphedema. Rather, resection of the cribriform fascia begins over the area of femoral pulsation, exposing the underlying femoral vessels. A few small branches of the femoral nerve are sacrificed during this dissection. The sheath of the femoral artery is incised along its anteromedial aspect from somewhere between the base of the fossa ovalis and the apex of the femoral triangle to its emergence from under the inguinal ligament. Branches, such as the external pudendal artery, are ligated as they are encountered. There is no purpose in dissecting under the artery or between the femoral artery and vein. Rather, the dissection that has been performed over the top of the artery is continued over the top of the vein, mobilizing the specimen to the medial aspect of the femoral vein. During this process, the saphenofemoral venous junction is identified, ligated with a 2-0 silk free-tie followed by a suture ligature for security, and transected, thus removing several centimeters of the saphenous vein with the specimen (Fig. 49.17E).
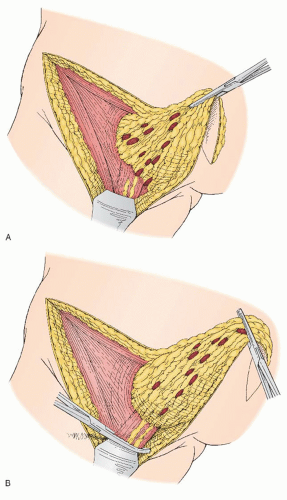 FIGURE 49.17 A: Inguinal-femoral lymphadenectomy. The corner of the groin specimen is dissected up from lateral to medially off the sartorius muscle. The lateral portion of fossa ovalis and cribriform fascia are exposed. B: The block of lymph node-bearing tissue has been mobilized, and the fatty lymphatic tissue overlying the saphenous vein is clamped. |
ligament superiorly, and from the underlying pectineal fascia. Dissection is continued toward and off of the adductor longus fascia until the labiocrural fold is reached (Fig. 49.17F).
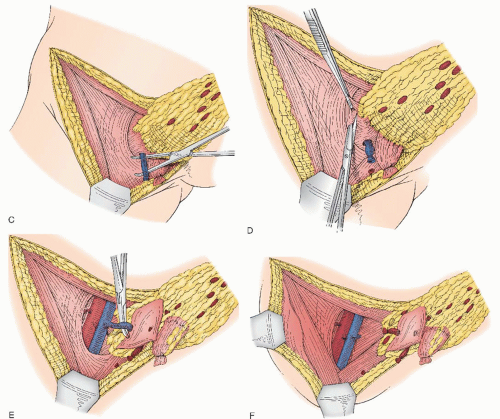 FIGURE 49.17 (Continued) C: The saphenous vein is identified, isolated, clamped, and divided near its entrance into the femoral triangle. D: Dissection of the femoral lymph nodes beginning with the separation of the cribriform fascia and the contents of the fossa ovalis from the anterior aspect of the femoral artery. E: The groin specimen containing the fatty nodal tissue above the cribriform fascia and the femoral nodes below the cribriform fascia are reflected medially exposing the femoral vessels and the insertion of the saphenous vein. F: The saphenous vein has been divided and ligated. The nodal tissue bundle is then completely excised and removed. The femoral triangle has been cleared of all nodal tissue. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


