Developing Leadership in Global Child Health
Yet despite a 30% decline in childhood deaths around the world from 1990 to 2009, the United Nations Children’s Emergency Fund (UNICEF) still reports 8.1 million deaths in children under the age of 5 in 2009 [1]. Approximately 70% of these deaths are preventable by available knowledge and technology [2]. Therefore, 5.5 million deaths in children can be prevented by what we know and have available to us. These simple questions still exist: Why do these deaths occur when we know how to prevent them? How can we reduce the gap between our knowledge base and our actions leading to these poor health outcomes?
What is known about global child health leadership? The unfortunate answer is: not very much.
Primary health care
In 1978, Primary Health Care (PHC) was launched at Alma Ata with the slogan “Health for All by the Year 2000” [3]. PHC aimed to create national health systems, based on the economic abilities of each country [4]. The type of health care employees would be dependent on each country’s goals and resources available.
The specific Alma Ata declaration aimed to increase the participation of community members in the development of health care, and aimed to decentralize health care to individuals at a local level [3].
The key principles can be summarized as follows: (1) PHC aimed to promote equity within health care; (2) community participation was paramount at all decision-making points; (3) prevention was highlighted over cure; (4) available technology should be used; (5) other sectors should be involved in health care (such as education, agriculture and housing); (6) decentralization of decision-making was important; and (7) leadership was needed to achieve the goals of PHC [5].
The Millennium Development Goal #4: reducing child mortality
The fourth Millennium Development Goal (MDG #4) is to reduce the under-5 mortality rate by two-thirds from 1990 to 2015 [6]. We have seen the number of children dying from developing countries decrease from 100 (1990) to 72 (2008) deaths per 1000 live births, with only 10 of 67 countries with high child mortality on track to meet the MDG target [7]. The continuing challenge, however, has been the slow decline in childhood deaths in sub-Saharan Africa, with high fertility rates and a slow reduction in under-5 mortality rates (Fig. 1).
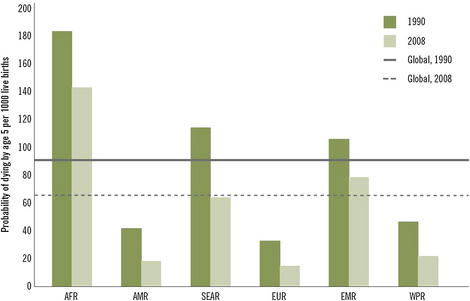
Fig. 1 Mortality rate in children younger than 5 years by WHO region.
(Reprinted from www.who.int/whosis/whostat/EN_WHS10_Part1.pdf, p. 13; copyright The World Health Organization; with permission.)
Other associated MDG #4 objectives include reducing the infant mortality rate, and increasing the proportion of 1-year-old children immunized against measles (Fig. 2).
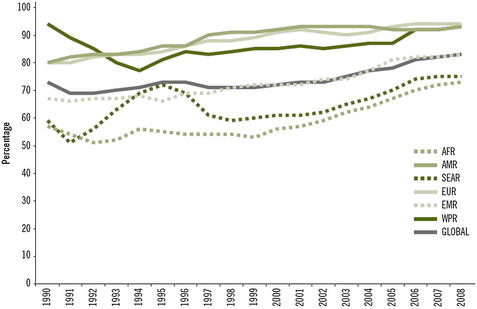
Fig. 2 Measles immunization coverage among 1-year-olds by WHO region.
(Reprinted from www.who.int/whosis/whostat/EN_WHS10_Part1.pdf, p. 14; copyright The World Health Organization; with permission.)
There are obvious trends downward in the number of childhood deaths. There have been large falls in under-5 mortality rates across all areas of the world, but because of high fertility rates, there has been little progress in overall numbers of childhood deaths in sub-Saharan Africa [7].
Why are we failing to reduce child deaths faster?
As far back as David Morley’s classic textbook on global child health, Paediatric Priorities in the Developing World, there was widespread recognition that improvements in children’s health were not strictly rooted in medical answers [8]. The challenge is that many of the underlying root causes of child deaths are not simple and straightforward medical causes that health professionals tackle on a daily basis. For example, poverty, poor female education, and poor water and sanitation remain barriers to successfully reducing childhood mortality.
Regarding the solution to global child health mortality, the technical aspects are not the problem as much as access to health care. For example, one area where there has been little reduction in global child mortality in the past decade has been on perinatal mortality. The challenge remains in identifying mothers who will run into trouble, getting access to the right level of care, and ensuring the quality of care once they arrive at the facility [9].
Our current global child health leaders continue to face a combination of economic, policy and political challenges to improve health systems and health outcomes for children. In particular, a cadre of child health leaders who can advocate for children and policy change should be developed in the existing health care system. Leveraging existing collaborative networks, such as the Program for Global Pediatric Research, can bring together child health leaders from Africa and around the world to forward the global child health agenda [10].
What is leadership?
There is great difficulty in defining what leadership is. Is it experience? Is it logic? Is it vision? Pulitzer Prize winner James MacGregor Burns, in his influential book Transforming Leadership, aptly states: “I have come to see leadership not only as a field of study but as a master discipline that illuminates some of the toughest problems of human needs and social change” [11]. The reality is that leadership occurs at various levels, both from positions of power and from individuals at the grassroots level.
Leaders such as Gandhi in India, Mao Tse-Tung in China, and Alexander the Great are well-known leaders who helped transform countries and societies. The question is whether the intrinsic characteristics of an individual, the “Great Man” theory proposed by Sidney Hook, “creates” leadership through the natural intellect and strength of character [12]. Countervailing ideas suggest that leadership may be a product of time and circumstances, and by decisions made at opportune times. This idea was championed by Karl Marx [13] and later by the philosopher, Herbert Spencer [14]. In particular, Spencer championed the concept that complex influences were what created the conditions by which leaders, through a Darwinian process, would succeed through the creation of wealth and power. So the concept of a great leader was hypothesized either to be intrinsic to the leader oneself, or a concept dependent on the circumstances and the situation. Thus, leadership can also occur at local levels around specific issues that lead to direct activism, such as protecting women from being sexually exploited or by protecting a local park or forest from being harmed.



