Fig. 1.1
Beaver handle with a no. 69 blade
Retroperitoneal Approach
This approach may be performed with the patient in either a prone, lateral, or even supine position. The approach with the patient in the prone position is described here, as it is the preferred method of the authors.
Anesthesia
General anesthesia should be used via endotracheal intubation; the muscles should be relaxed.
Patient Position
The patient is placed in a prone position. A bolster/sandbag is placed under the pelvis and lower chest so that the renal angle is opened out. This space is bordered inferiorly by the iliac crest, medially by the lateral border of the sacrospinalis, and superiorly by the 11th and 12th ribs (Fig. 1.2 ). Too much elevation will result in approximation of the ribs and the iliac crest, thereby reducing the working space. A useful way of ascertaining adequate support and elevation is by passing a hand below the elevated trunk. Easy passage of the upturned palm indicates adequate positioning. The renal angle may be further opened out by slightly abducting the entire pelvis away from the affected side. Finally the patient should be positioned as shown in Fig. 1.2 at the very edge of the table on the affected side to allow easy maneuverability of the instruments. The arms and legs should be well supported and padded (Fig. 1.3 ).
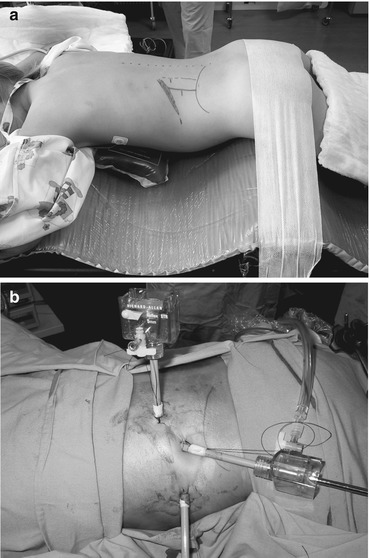
Fig. 1.2
Landmarks and boundaries of the renal space: ribs (R), sacrospinalis (S), and iliac crest (I)
Fig. 1.3
(a) Patient position for prone retroperitoneoscopic nephrectomy and (b) the ports in situ
Access
The primary port is inserted at the lateral border of the sacrospinalis midway between the iliac crest and the 12th rib. A 5 mm/10 mm incision, depending on the size of port, is made in the skin. A blunt artery forceps, such as a Dunhill forceps, is “walked” off the lateral border of the sacrospinalis through the dorsolumbar fascia until the perinephric area is reached. This is evidenced by a sudden give through the muscle and free movement of the forceps. A ready-made balloon device or the middle finger of an 8.5 glove tied to a 12Fr Nelaton catheter with a three-way tap and 50 ml Luer-Lok syringe is inserted into the perinephric space (the authors’ preference) (Fig. 1.4 ). The balloon is blown up gradually to approximately 200 ml. Too rapid inflation may result in rupture of the balloon. Alternatively, the port may be inserted and the space created using the telescope itself. Once the balloon is deflated, the balloon is removed and the port inserted. The working ports are placed just inferior to the tip of the 11th rib, and, if required, a second working port is placed under vision through the sacrospinalis muscle either in line with or superior to the primary port. The insufflation pressure is maintained at 10–12 mmHg at a flow rate of 1 l/min [5].

Fig. 1.4




Inexpensive balloon dissector made with the middle finger of an 8.5 glove tied to a 12 Fr Nelaton catheter, a three-way tap, and a 50 ml Luer-Lok syringe
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
