Fig. 25.1
Appearances on micturating cystourethrogram
While the child is on catheter drainage, biochemical parameters are monitored, awaiting stabilization of renal function and achievement of a nadir creatinine level. Following catheterization, the child may go through a phase of post-obstructive diuresis. Therefore, fluid and electrolyte balance should be carefully monitored. Any concurrent urinary tract infection is treated with antibiotics.
In cases where there is significant renal impairment, the input of a pediatric nephrologist is extremely valuable. Following a period of stabilization (usually 10 days to 2 weeks), when the child is hemodynamically and biochemically stable, the obstructing valve membrane is ablated.
Contraindications
To effectively deal with a large majority of infants with posterior urethral valves, appropriate endoscopy equipment must be available.
A relative contraindication to primary valve ablation would include premature infants, in whom the urethra is not of sufficient caliber to accommodate even the smallest of the pediatric endoscopes. The options available in this situation include a temporary diversion with the vesicostomy or, alternatively, one could try and serially dilate up the urethra by passing increasing caliber urethral catheters over a 2- to 4-week period.
In the past, other techniques have been described to ablate the obstructing leaflets. These include a suprapubic transvesical endoscopic approach through the bladder neck, ablation via a temporary perineal urethrostomy, Fogarty balloon ablation, and using Whitaker’s hook. The availability of miniature endoscopes has made these techniques redundant [6, 7].
Preoperative Investigation
Prior to resection of the posterior urethral valve membrane, ensure that the child is hemodynamically and biochemically stable. Specifically, one should check the serum values of creatinine, electrolytes, and acid–base balance to ensure that the child is not acidotic. Radiological confirmation of the diagnosis with ultrasound and MCUG is arranged prior to endoscopy.
Specific Instrumentation (See Figs. 25.2 and 25.3)
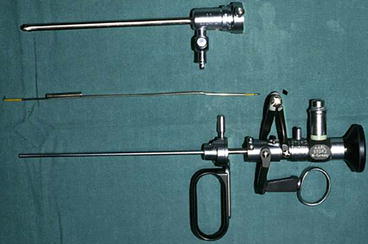
Fig. 25.2
Resectoscope

Fig. 25.3
Cold knife and diathermy hook
Instruments that should be available for valve resection include:
1.
Pediatric cystoscope (6 F–7.5 F)
2.
Pediatric resectoscope (11 F)
3.
Cold knife, bugbee, and diathermy electrodes
Operative Technique
The child is placed in a lithotomy position. Prior to instrumentation, a dose of intravenous antibiotic covering the gram-negative spectrum of organisms is administered (usually gentamicin or amikacin).
The foreskin is separated to retract and visualize the meatal opening. The meatus is calibrated and if necessary serially dilated. An initial diagnostic cystoscopy is performed. I use the 6 F–7.5 F graduated Wolfe cystoscope, which has an inbuilt 30° telescope and a 3/4 F instrument channel.
Following the initial assessment, the valve ablation is carried out using a pediatric 11 Fr resectoscope, with a cold knife or a bugbee electrode. The advantage of the 11 F resectoscope (Storz) is that the tip of the sheath has no bakelite beak and is thus less traumatic and easier to introduce.
In situations where the neonatal urethra is too small to accommodate the resectoscope, the membrane can be ablated using the 7.5 F cystoscope and a 3 F bugbee electrode using a diathermy current.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


