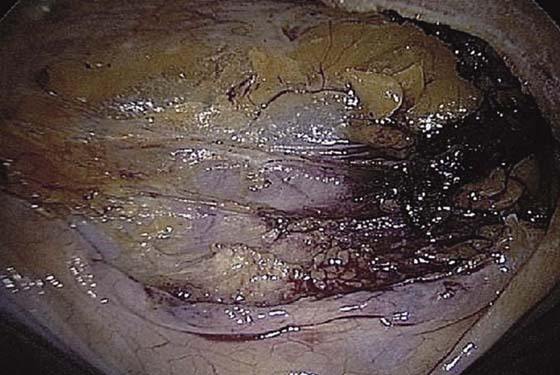
CHAPTER 119 Mark D. Walters Laparoscopic Burch colposuspension is one of the primary surgical treatment options for stress urinary incontinence. Cure rates appear to be similar to open Burch colposuspension in most studies, although studies with long-term follow-up are not available. Several reviews of the literature on laparoscopic Burch colposuspension have been published. Laparoscopic Burch colposuspension can be done using an extraperitoneal or an intraperitoneal approach. The intraperitoneal approach to the Burch colposuspension begins with insertion of the laparoscope through a 5- to 10-mm intraumbilical trocar, followed by intra-abdominal insufflation. Inspection of the peritoneal cavity is performed, delineating the inferior epigastric vessels, abdominal and pelvic organs, and any abdominal or pelvic pathology. Two additional trocars (5 mm and 5/12 mm) are placed under direct vision, one on each side in the lower abdomen. The bladder is filled with 200 to 300 mL sterile water or saline. A probe can be used to press the base of the bladder upward so that the upper margin of the bladder is easily delineated (Fig. 119–1). Using sharp dissection with electrocautery or a harmonic scalpel, a transverse incision is made 2 cm above the bladder reflection between the median umbilical ligaments (Fig. 119–2). Blunt and sharp dissection aiming toward the posterior/superior aspect of the pubic symphysis decreases risk of bladder injury. Identification of the areolar tissue at the point of incision confirms a proper plane of dissection (Fig. 119–3). Blunt dissection is then carried out inferolaterally on both sides to identify the pubic symphysis, Cooper’s ligaments, obturator internus muscles, arcus tendineus fasciae pelvis, and bladder neck (Fig. 119–4). Midline dissection over the urethra should be avoided. FIGURE 119–1 The bladder is filled before the Burch colposuspension is begun. The upper margin of the bladder can be delineated by pressing up on the base of the bladder. FIGURE 119–2 Sharp dissection is used to incise the peritoneum 2 cm above the bladder reflection. FIGURE 119–3 Identification of areolar tissue at the point of incision confirms the proper plane of dissection.
Laparoscopic Surgery for Stress Urinary Incontinence (Burch Colposuspension)
 Tommaso Falcone
Tommaso Falcone


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


