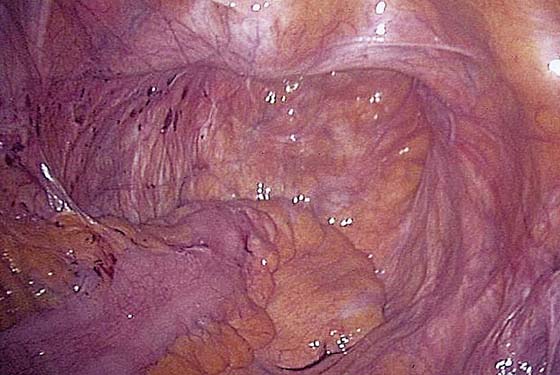
CHAPTER 120 Mark D. Walters In addition to the intraumbilical port, a 5/12-mm trocar should be placed in both lower quadrants for suture introduction. One or two additional 5-mm ports are placed at the level of the umbilicus lateral to the rectus muscle for retraction. The deep pelvis is then visualized, noting the pelvic structures and central enterocele (Fig. 120–1). A sponge stick or obturator is placed in the vagina to elevate the vaginal apex (Fig. 120–2). The peritoneum is dissected off the vaginal apex to delineate the vaginal wall and endopelvic fascia. Anterior dissection is performed as needed, taking care to avoid damage to the bladder (Fig. 120–3). We dissect the peritoneum from the posterior vaginal wall as deeply as possible in the rectovaginal space, sometimes extending almost to the perineal body. Occasionally, a lubricated sponge stick can be placed in the rectum, as well as in the vagina, to delineate both of these structures (Fig. 120–4). A 15 × 2.5-cm strip of polypropylene mesh is introduced through the 5/12-mm port. Three or four pairs of permanent sutures are placed to attach the mesh to the distal two thirds of the posterior vaginal wall (mesh should be attached as close to the perineal body as possible) (Fig. 120–5). An additional small strip of mesh is connected to the anterior vaginal wall near the apex using two pairs of permanent sutures. The posterior and anterior meshes can then be connected at the vaginal apex, forming a Y- or T-shaped mesh. An alternative technique is to fashion the Y-shaped mesh extracorporeally and then bring it into the abdomen for suturing. Care should be taken to avoid twisting of the mesh and tangling of the sutures. Fig. 120–6 illustrates the completed vaginal mesh attachment. The mesh is then elevated, and the uterosacral ligaments are plicated in the cul-de-sac below the mesh using permanent sutures. One to three sutures may be necessary (Fig. 120–7). Alternatively, a Moschcowitz or Halban procedure can be done. The peritoneum over the sacral promontory then is examined, and key structures such as the aortic bifurcation, iliac arteries and veins, and right ureter are visualized. The peritoneum over the sacral promontory is carefully incised longitudinally, and, using elevation and blunt dissection, the sacral promontory is exposed (Fig. 120–8). The surgeon should identify the middle sacral artery and vein. A 3- to 4-cm section of anterior sacrum should be exposed if possible. The peritoneum running down the right pararectal space should be opened toward the cul-de-sac as well. Special care should, of course, be taken to avoid the ureter. Two to three permanent sutures are used to attach the mesh to the sacral promontory using extracorporeal knot-tying (Fig. 120–9). Alternatively, titanium tacks or hernia staples may be used to attach the mesh to the anterior longitudinal ligament of the sacrum. The peritoneum is then closed over the mesh using running or interrupted sutures (Fig. 120–10). FIGURE 120–1 The deep pelvis is visualized in a woman with vaginal prolapse and a central enterocele.
Laparoscopic Surgery for Pelvic Organ Prolapse
 Tommaso Falcone
Tommaso Falcone
Laparoscopic Sacral Colpopexy

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


