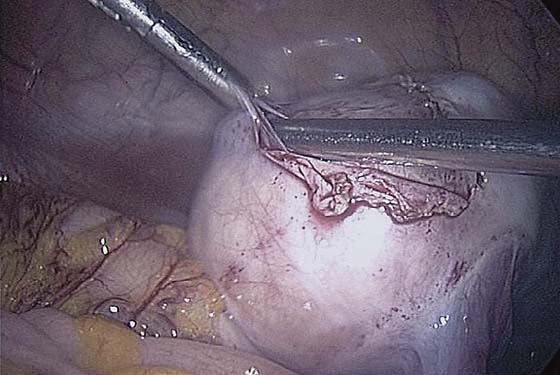
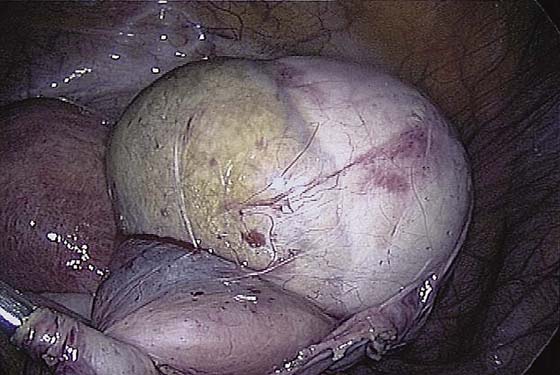
CHAPTER 118 Tommaso Falcone Ovarian cystectomy is the treatment of choice for the conservative management of ovarian cysts presumed to be benign. Simple aspiration is associated with a high recurrence rate, and cyst fluid cytology is unreliable. Transvaginal ultrasonography is used to evaluate an ovarian cyst. High-risk criteria on ultrasonography for predicting the pathologic diagnosis, such as a cystic-solid mass or ascites, are a contraindication to laparoscopic surgery unless a dermoid or endometriosis is suspected. A preoperative CA-125 level is useful in postmenopausal, but not in premenopausal, women. The same principle applies to Doppler flow assessment. Magnetic resonance imaging (MRI) does not help in distinguishing a malignant from a benign mass. An attempt should be made to remove the cyst without rupture. Equivalent rates of rupture are found with laparotomy and laparoscopy. Rupture of a dermoid cyst does not appear to be associated with any short-term complications if copious irrigation is used. Intraoperative rupture of stage I ovarian carcinomas does not appear to affect prognosis. The patient should have consented to a laparotomy if a cancer is found. Pneumatic compression stockings are placed on the calves. An orogastric tube is used if stomach distention is suspected. An examination is carried out with the patient under anesthesia, and a Foley catheter is inserted. To perform ovarian cystectomy, the standard three-puncture technique is used. The peritoneal cavity is systematically assessed as described in Chapter 116. Peritoneal fluid should be obtained for cytology. If no excrescences or peritoneal signs of malignancy are present, the surgeon can proceed with the cystectomy. The ovarian cortex is coagulated, and an incision is made (Fig. 118–1). The edge of the cortex is grasped with an Allis forceps and dissected from the cyst. The cyst can be separated from the cortex with blunt dissection using the suction-irrigation device (Fig. 118–2). The cyst is then enucleated from the ovary (Fig. 118–3) and is placed into the anterior cul-de-sac (Fig. 118–4). Bipolar cautery is used to achieve hemostasis from any blood vessels encountered. Once the cyst is ready to be removed from the peritoneal cavity, it is placed in a bag (Fig. 118–5). The bag is then brought up to the skin, and the cyst decompressed within it (Fig. 118–6). The cyst can then be morcellated out of the bag. The ovarian cortex is not usually closed, but a simple suture can be applied to close a deep defect. FIGURE 118–1 The ovarian cortex is coagulated and incised. FIGURE 118–2 A suction-irrigation device is used to get a plane of dissection between the cortex of the ovary and the cyst. FIGURE 118–3 The cyst is dissected from the ovary with a traction-countertraction technique. FIGURE 118–4 The cyst is placed in the cul-de-sac so that the ovary can be inspected for bleeding. FIGURE 118–5 The cyst is placed in the bag prior to removal. FIGURE 118–6 The bag is brought through a port site. Most of the bag remains within the peritoneal cavity. The cyst is ruptured within the bag, the contents suctioned, and the solid parts removed in pieces. A salpingo-oophorectomy is the treatment of choice for ovarian cysts found in perimenopausal and postmenopausal women because the chance of rupture is reduced substantially. The same preoperative and intraoperative preparation as for the cystectomy is performed prior to a salpingo-oophorectomy. A retroperitoneal approach is recommended. The technique of ovarian salpingo-oophorectomy is as follows. The peritoneum is incised lateral to the ovarian vessels, and the retroperitoneal space is identified (Fig. 118–7). Blunt dissection is used to identify the ureter that is attached to the medial leaf of the broad ligament (Fig. 118–8
Laparoscopic Adnexal Surgery
 Mark D. Walters
Mark D. Walters
Ovarian Cystectomy



Salpingo-oophorectomy
![]()
Stay updated, free articles. Join our Telegram channel


Full access? Get Clinical Tree


