Intussusception
Intussusception is the most frequent cause of bowel obstruction in infants and toddlers. It is an acquired invagination of the proximal bowel (intussusceptum) into the distal bowel (intussuscipiens). It was first described in 1674 by Paul Barbette of Amsterdam, defined by Treves in 1899, and operated on successfully in 1873 by John Hutchinson.1,2
Pathophysiology
Primary Intussusception
The vast majority of cases do not have a lead point and are classified as primary or idiopathic intussusceptions. The cause is generally attributed to hypertrophied Peyer patches within the bowel wall.3 Intussusception occurs frequently in the wake of an upper respiratory tract infection or an episode of gastroenteritis, providing an etiology for the hypertrophied lymphoid tissue. Adenoviruses in children older than age two, and to a lesser extent rotaviruses, have been implicated in up to 50% of cases.4,5 Other contributing evidence that viruses may play a role in intussusception includes the rise in cases during seasonal respiratory viral illnesses and the increased risk associated with previous rotavirus immunization.6 The newest immunization formulas available in the USA, RotaTeq® and Rotarix®, have not been associated with intussusception in both pre- and post-marketing studies.6–10
Secondary Intussusception
An intussusception may have an identifiable lesion that serves as a lead point, drawing the proximal bowel into the distal bowel by peristaltic activity. The incidence of a lead point varies from 1.5% to 12% and the presence of a lead point increases in proportion with age.11,12 The most common lead point is a Meckel diverticulum followed by polyps and duplications. Other benign lead points include the appendix, hemangiomas, carcinoid tumors, foreign bodies, ectopic pancreas or gastric mucosa, hamartomas from Peutz–Jeghers syndrome (Fig. 38-1), and lipomas. Malignant causes, although rare, increase in incidence with age and include lymphomas and small bowel tumors.13 Systemic diseases, including Henoch–Schönlein purpura and cystic fibrosis, have been associated with intussusception. Other rare diseases related to intussusception are celiac disease and Clostridium difficile colitis.14

FIGURE 38-1 (A) Operative view of the outside of the jejunum shows a palpable mass as the lead point of a reduced intussusception. (B) A hamartomatous polyp is characteristic of Peutz–Jeghers syndrome. (C) Mucocutaneous macular lesions are seen in this patient with Peutz–Jeghers syndrome. Note extension of the pigmentation beyond the vermilion border.
Incidence
Idiopathic intussusception can occur at any age. Most patients are well-nourished, healthy infants, and approximately two-thirds are boys. The highest incidence occurs in infants between ages 4 and 9 months,15 and it is also the most common cause of small bowel obstruction in this age group.16 Intussusception is uncommon below 3 months and after 3 years of age. The condition has been described in premature infants where it has been postulated as the cause of small bowel atresia in some cases.17
Clinical Presentation
The classic presentation is an infant or a young child with intermittent, crampy abdominal pain associated with ‘currant jelly’ stools and a palpable mass on physical examination, although this triad is seen in less than a fourth of children.18 The abdominal pain is sudden and the child may stiffen and pull the legs up to the abdomen. The pain can also be associated with hyperextension, writhing, breath holding and vomiting. The attack often ceases as suddenly as it started. Between attacks, the child may appear comfortable but eventually will become lethargic. Small or normal bowel movements will stop as the obstruction progresses and becomes associated with bilious emesis and increasing abdominal distention. Stools may be blood tinged as impending ischemia causes mucosal sloughing and compression of mucous glands leading to evacuation of dark, red mucoid clots or ‘currant jelly’ stools. This is often a late sign as are laboratory derangements. A pitfall is to wait for the currant jelly stool, leukocytosis, and electrolyte abnormalities that are often hallmarks of ischemic bowel.
Physical Examination
The child’s vital signs are usually normal early in the disease course. During painless intervals, the child may appear comfortable and the physical examination may be unremarkable. However, the cramping episodes usually occur every 15 to 30 minutes and re-examination may prove difficult. There may be audible peristaltic rushes, and a sausage-shaped or curved mass might be palpable anywhere in the abdomen or even visualized if the child is relatively thin (Fig. 38-2). The right lower abdominal quadrant can appear flat or empty (Dance sign) as the intussuscepted mass is drawn cephalad. On rectal examination, bloodstained mucus or blood may be encountered as a later sign. If the obstructive process worsens and bowel ischemia occurs, dehydration, fever, tachycardia, and hypotension can develop in quick succession as a result of bacteremia and bowel necrosis.
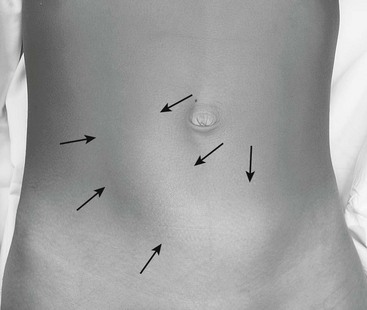
FIGURE 38-2 This 10-year-old boy has a palpable sausage-shaped mass (arrows) due to an intussusception.
Diagnosis
Abdominal Radiography
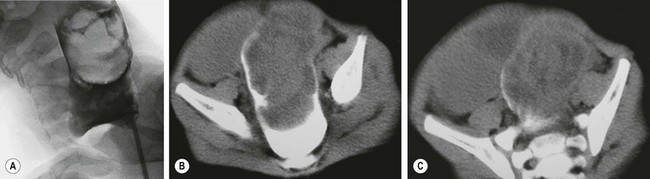
In half of cases, the diagnosis of intussusception can be suspected on plain flat and upright abdominal radiographs (Fig. 38-3). Suggestive radiographic abnormalities include an abdominal mass, abnormal distribution of gas and fecal contents, sparse large bowel gas, and air-fluid levels in the presence of bowel obstruction. However, plain films have limited value in confirming the diagnosis and are not used as the sole diagnostic test. They are best utilized as a screening tool when one of the abnormal findings listed above is found.19

Ultrasonography
The use of abdominal ultrasound (US) for the evaluation of intussusception was first described in 1977.20 Since then, most institutions have adopted it as a screening tool because of the lack of radiation exposure, ability to identify pathologic lead points, and decreased cost.21,22 The characteristic finding on ultrasound has been referred to as a ‘target’ or ‘doughnut’ lesion (Fig. 38-4), which consists of alternating rings of low and high echogenicity representing the bowel wall and mesenteric fat within the intussusceptum in a transverse plane. The ‘pseudokidney’ sign is seen on longitudinal section (Fig. 38-5). This pattern is secondary to the edematous walls of the intussusceptum within the intussuscipiens. Ultrasonography can also guide the therapeutic reduction of an intussusception.21 Equivocal findings using this modality should mandate a conventional contrast or air enema.23

FIGURE 38-4 This transverse sonographic image shows the alternating rings of low and high echogenicity due to an intussusception. This finding has been called a ‘target’ sign.

Computed Tomography and Magnetic Resonance Imaging
Neither computed tomography (CT)24 nor magnetic resonance imaging (MRI) are routinely used in the evaluation of a patient with intussusception, although either may confirm this diagnosis and/or pathologic causes for intussusception, such as a malignancy (i.e., lymphoma). The characteristic CT finding is a ‘target’ or ‘doughnut’ sign (Fig. 38-6). Transient small bowel intussusceptions that are discovered on CT or MRI are usually not clinically significant.21 Radiographic or operative treatment should be based on clinical findings in symptomatic patients.25 Laparoscopy is an excellent means to evaluate these patients if surgical intervention is needed.