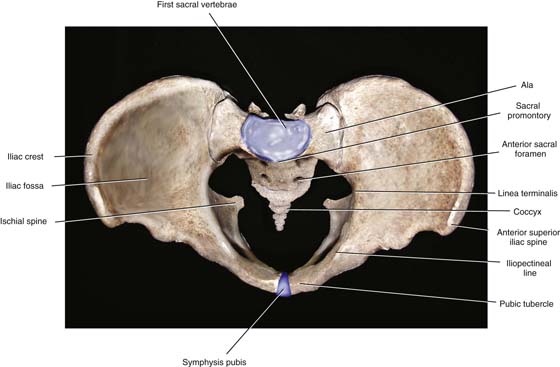
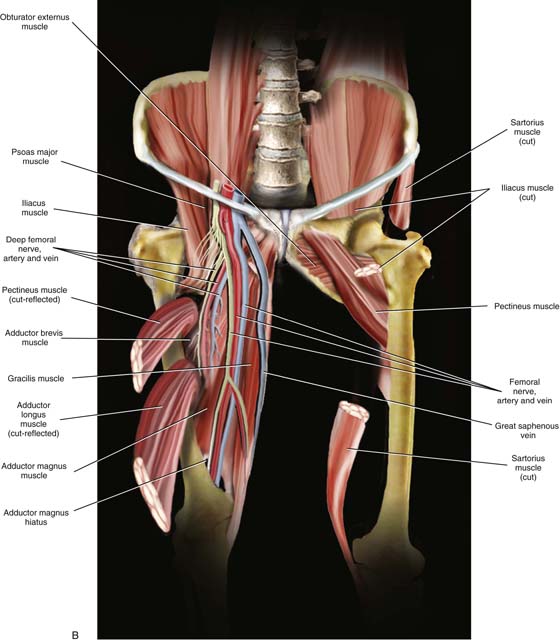
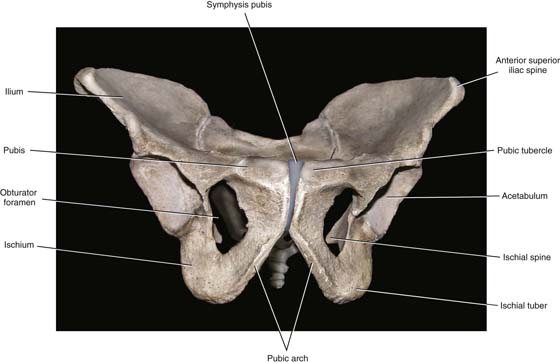
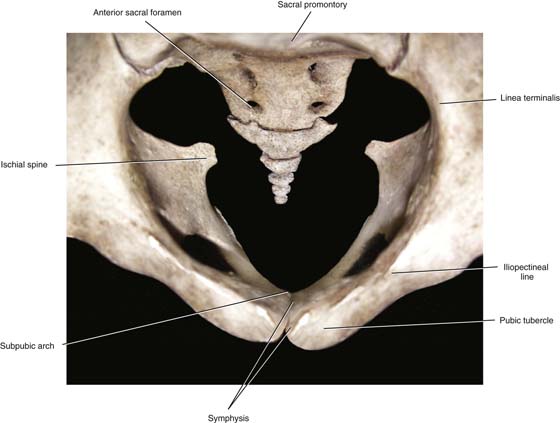
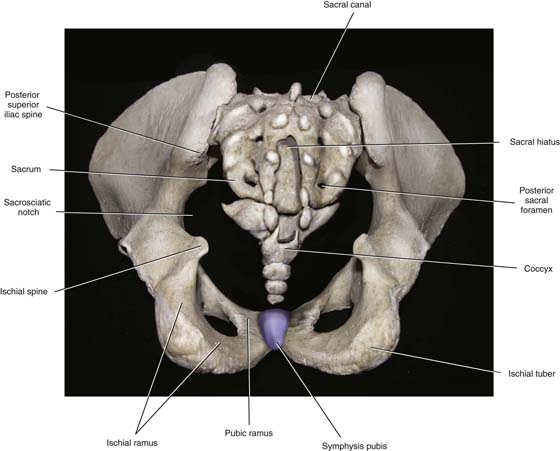
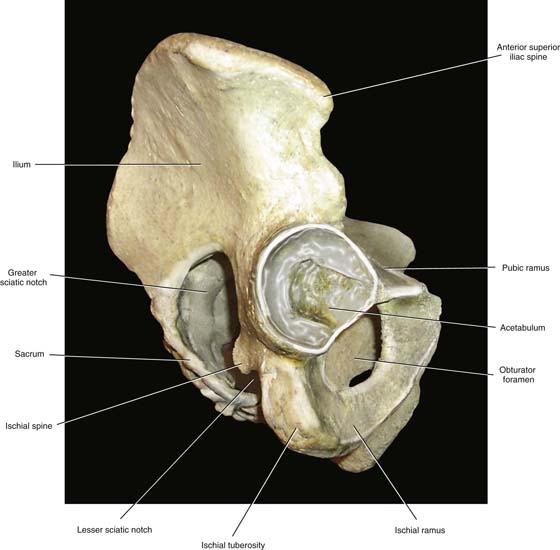
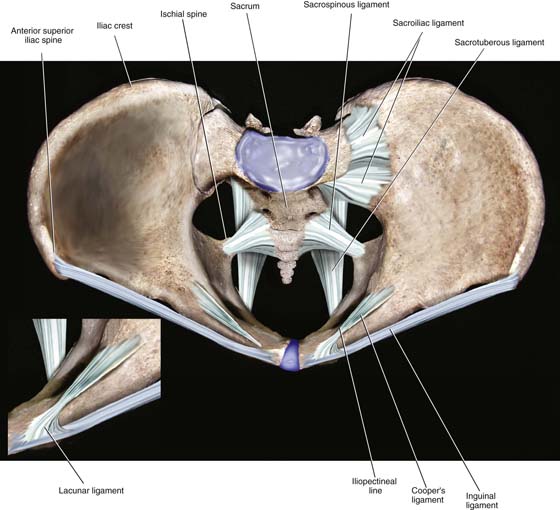
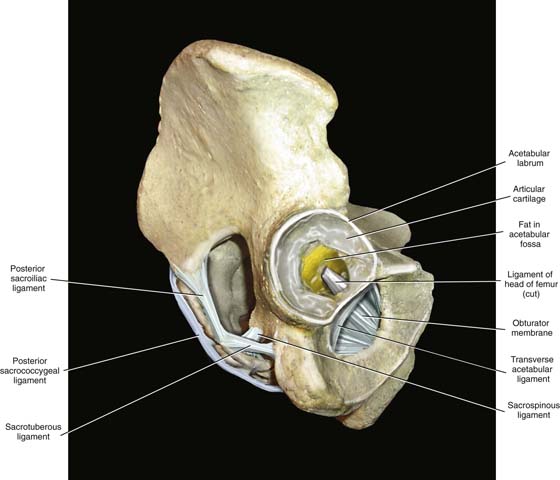
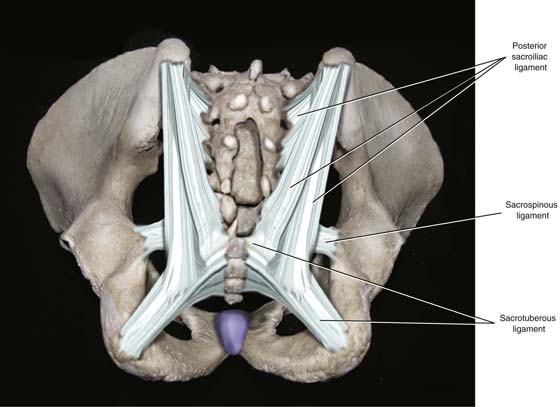
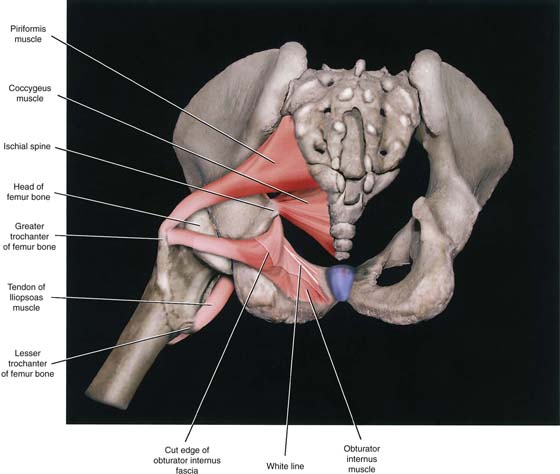
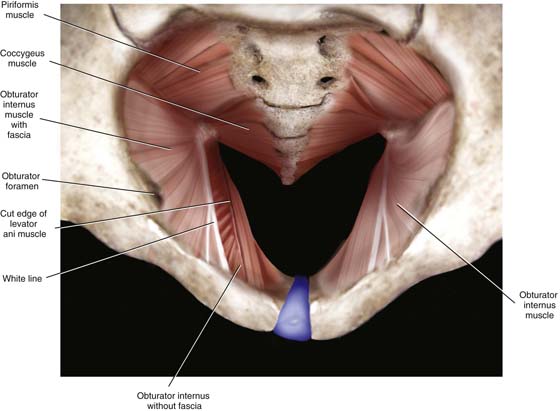
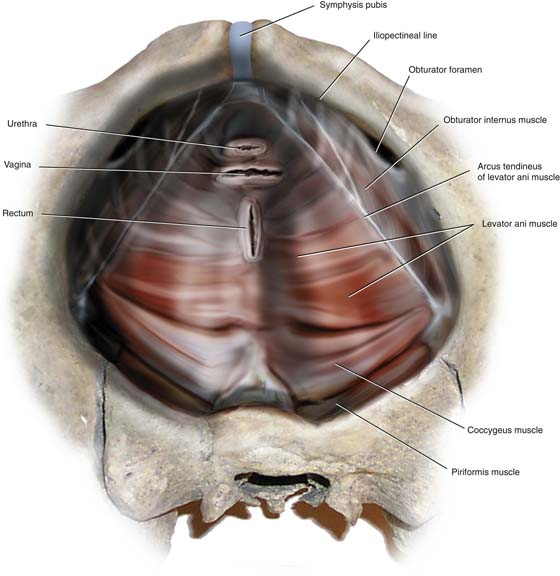
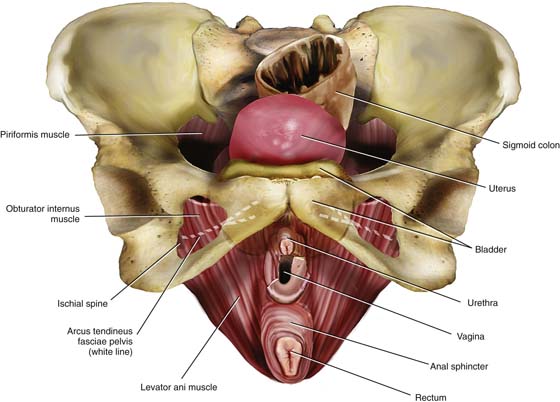
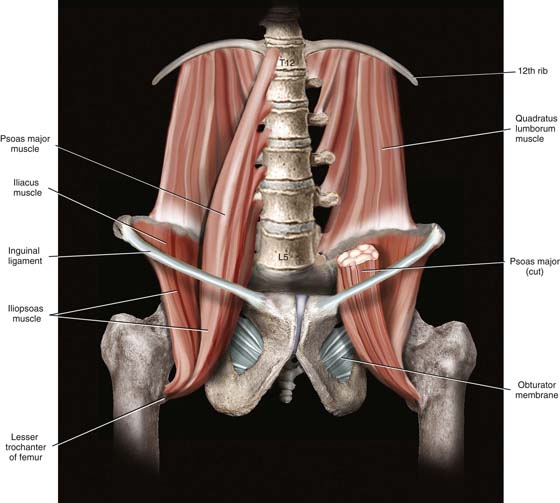
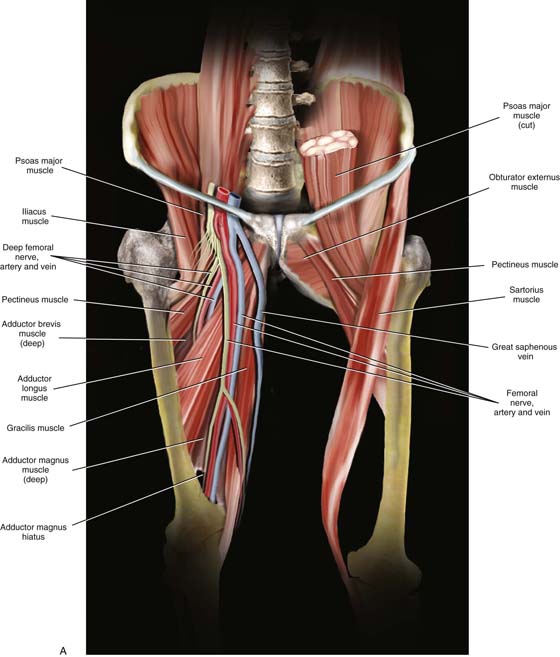
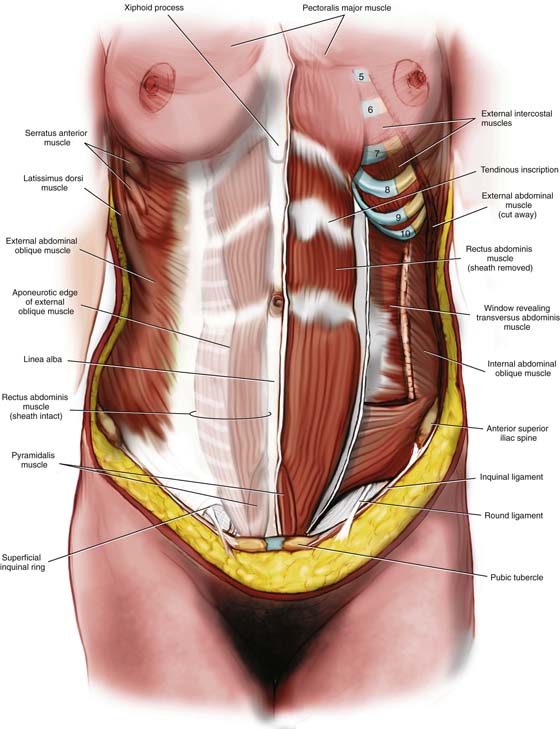
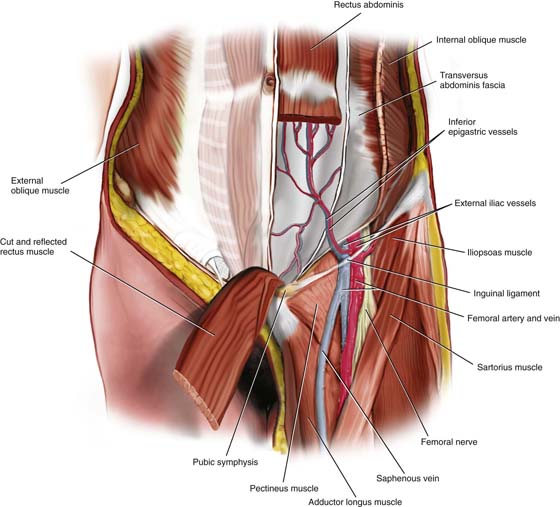
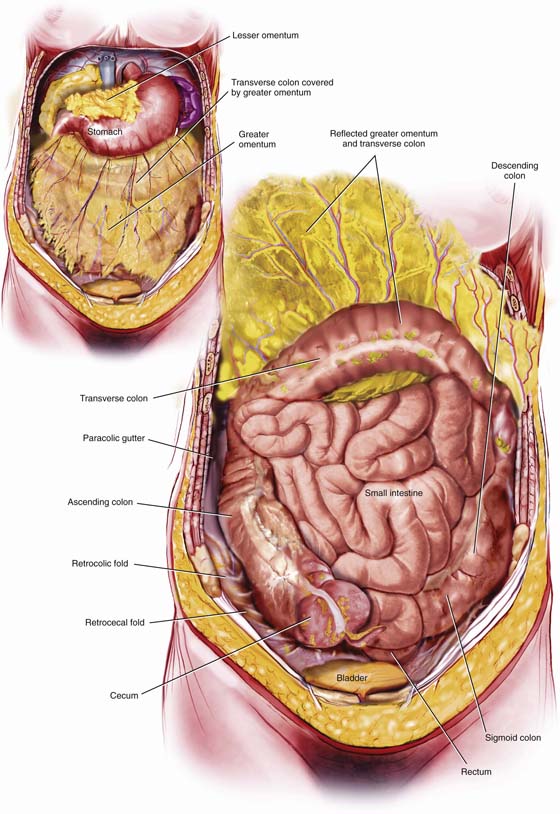
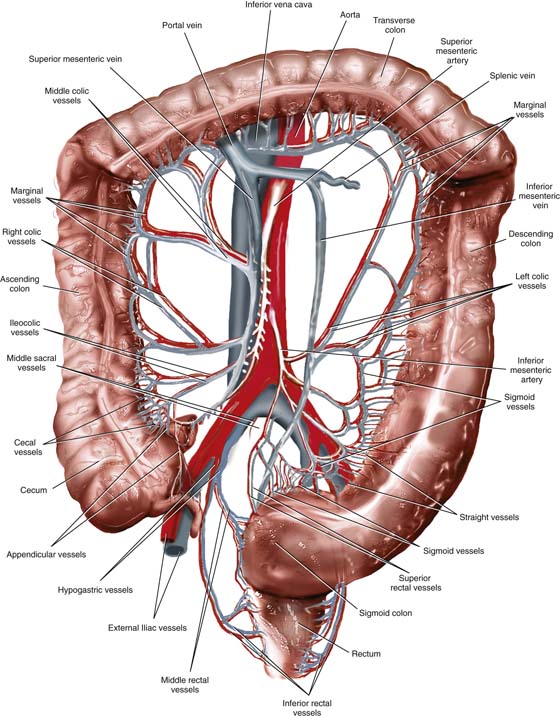
CHAPTER 1 The anatomy taught in this book is based on actual cadaveric dissection. This section consists entirely of color drawings constructed from anatomic models (cadavers). This section was added to help the reader orient the dissection photographs to the overall geography of abdomen, pelvis, breasts, and extremities. In several pictures, our artist has used actual photographs of body parts (pelvic bone) into which muscles and ligaments were sketched via computer. The following terms are used in this section to provide directive relationships: (1) cranial = toward the head; (2) caudal = toward the foot; (3) superior = above; (4) inferior = below; (5) deep = to the interior; (6) superficial = to the surface; (7) medial = toward the midline; (8) lateral = toward the side; (9) beneath = under; (10) anterior = to the belly; and (11) posterior = to the back. The surgeon needs to be familiar with certain bony landmarks. The pelvic bones consist of the sacrum and coccyx, the ilium, the pubic bone, and the ischium (Fig. 1–1). The first anterior projection of the sacral vertebra is the sacral promontory, and the exaggerated transverse processes form the sacral ala (Fig. 1–2). On both anterior and posterior surfaces are the holes, or foramina, from which nerve roots exit. Articulating with the last sacral vertebra is the coccyx (Fig. 1–3). When the pelvis is observed from above (see Fig. 1–2), the iliac fossa, iliac crest, and anterior superior iliac spine are prominent. The articulations at the sacroiliac joint and the symphysis pubis mark major posterior and anterior joints, respectively. Between the two are the iliopectineal lines and the linea terminalis. Facing the pelvis, the anterior superior iliac spine and the pubic tubercle mark the boundaries of the inguinal ligament. The two pubic bones form an arch beneath the symphysis pubis. The rhomboid space between ischial and pubic bones is the obturator foramen (see Fig. 1–1). The lowest portion of the ischium forms a broad, rounded accumulation of bone referred to as the ischial tuberosity. Above that structure is a hemispherical socket (acetabulum), where the head of the femur articulates (see Fig. 1–1). When one faces the back of the pelvis, the sacrum and the sacral canal are visible. The ischial tuberosity, ischial spines, and greater and lesser sacral sciatic notches are identified (Fig. 1–4). From the side, the iliac crest, ischial tuberosity, ischial spine, greater sciatic notch, and lesser sciatic notch are seen, as is the obturator foramen (Fig. 1–5). The following ligamentous structures can be observed: Cooper’s ligaments, the sacroiliac ligaments, the symphysis fibrocartilage, the sacrospinous and sacrotuberous ligaments, the inguinal ligament, the lacunar ligament, and the obturator membrane (Figs. 1–6 through 1–8). The sacrospinous and Cooper’s ligaments are utilized in pelvic reconstructive surgery, as are the pubic symphysis and the anterior longitudinal ligament (overlying the anterior sacral surface, not sketched). Large vessels and nerves cross from the abdomen to the thigh beneath the inguinal ligament and through the obturator foramen. The lacunar ligament forms the medial abutment of the femoral canal and sometimes is referred to as the pectineal portion, or extension, of the inguinal ligament. The muscles of the pelvis that have practical and special importance for our discussion are the obturator internus muscle, which constitutes the “pelvic side wall” or “ovarian fossa,” the coccygeus, the piriformis, and the levator ani muscles (Fig. 1–9). The obturator fascia is a well-defined, tough structure. A particularly thickened portion of the obturator fascia is named the arcus tendineus, or white line (Fig. 1–10). The line stretches from the inner aspect of the ischial spine across the belly of the obturator internus muscle and terminates at the lower margin of the posterior pubic bone (Fig. 1–11). The levator ani muscle takes its origin from the inferior margin of the pubic bone and the entire arcus (obturator fascia). Several anatomy texts have divided the levator into anterior and posterior portions; however, these subdivisions are artificial and have little practical value (Fig. 1–12). Functionally, the gynecologist can feel this muscle contract by performing a rectovaginal examination and requesting the patient to tighten her muscles as if holding in a bowel movement. At a point 2 cm up (cranial) from the vaginal introitus, the U-shaped muscle is felt along the side and posterior vaginal walls. A similar contraction can be felt posterior to the rectum when the anal sphincter is contracted. Insofar as the rectum is concerned, the levator component can be palpated across the posterior rectal wall. The levator ani in concert with the external sphincter ani squeezes the rectum to narrow the bowel lumen while elevating the anorectum. The muscles and ligaments divide notches into windows (foramina). The coccygeus is overlain (deep) by the sacrospinous ligament. The piriformis muscle exits the pelvis via the greater sciatic foramen and is partially overlain (deep) by the sacrotuberous ligament (see Figs. 1–7 through 1–9). Internally, the hollow iliac fossa is covered by the iliacus muscle. At the medial margin and slightly superficial to the iliacus muscles are the psoas major muscles. Together with the iliacus (iliopsoas), the psoas major muscles pass into the thigh beneath the inguinal ligament to insert on the femur (lesser trochanter). Occasionally, the psoas minor tendon may be seen on the anterior surface of the psoas major muscle (Fig. 1–13). FIGURE 1–1 The pelvic bone consists of the ilium, ischium, and pubis. The ilium is bound to the sacrum at the sacroiliac joints. This anterior aspect of the pelvis shows the pubic arch, symphysis, and obturator foramen via a head-on view. FIGURE 1–2 This overhead view details the pelvic inlet, which is bounded anteriorly by the pubic symphysis and the pubic tubercle; laterally by the iliopectineal line and the linea terminalis; and posteriorly by the sacral alae and the first sacral vertebra. This view also nicely shows the ischial spines. FIGURE 1–3 High-power detail viewed through the pelvic inlet shows the sacrum and coccyx. The anterior sacral foramina are distinct, as are the ischial spines and the subpubic arch. FIGURE 1–4 The posterior view of the pelvis is combined with an outlet “looking-in” perspective. The ischial tuberosity, ischial spine, and greater and lesser sacrosciatic notches are best seen from this vantage point. Posterior sacrum highlights include the sacral hiatus, sacral canal, and posterior sacral foramina. FIGURE 1–5 This right lateral view depicts the acetabulum, sacrosciatic notches, anterior superior iliac spine, and ischium. FIGURE 1–6 The inguinal ligament stretches between the anterior superior iliac spine and the pubic tubercle. From the latter is reflected the lacunar ligament, which forms the medial boundary of the femoral canal. Cooper’s ligament is a stout structure that clings to the iliopectineal line (see inset). Between the ischial spines and the lateral aspect of the sacrum is the sacrospinous ligament. This ligament also creates the greater and lesser sacrosciatic foramina. FIGURE 1–7 This side view displays the obturator membrane, as well as the sacrotuberous ligament. The latter begins on the ischial tuberosity and terminates on the lateral margin of the sacrum. FIGURE 1–8 Posterior view combined with outlet view. The sacrotuberous ligament and the sacrospinous ligament cross. FIGURE 1–9 The ligaments have been eliminated. Views are through the pelvic outlet. The obturator internus, piriformis, and coccygeus are seen in sharp detail. FIGURE 1–10 The large obturator internus muscle covered with tough obturator fascia forms the pelvic sidewall. The arcus tendineus, or white line, is produced by a thickened area of obturator fascia. The levator ani muscle arises from the arcus. The cut edge of the levator is shown on the patient’s right side (viewer’s left side). The left levator has been removed. The enclosure of the pelvis is completed by the piriformis and coccygeus muscles. FIGURE 1–11 This view shows the intact levator ani muscle arising along the length of the arcus tendineus. Note the exposed retropubic space, together with the cut edges of the urethra and vagina. FIGURE 1–12 Frontal view of the funnel-like levator ani and its relationship to the vulva and superficial muscles of the perineum. The levator arises in part from the inferior margins of the pubic bone. The artist has superimposed the arcus tendineus (dashed white line) onto the obturator internus and pubic bone. FIGURE 1–13 The large muscles of the retroperitoneum include the psoas major muscle, iliacus muscle, and quadratus lumborum muscle. The psoas and iliacus (iliopsoas) depart the abdomen and enter the thigh beneath the inguinal ligament. The muscles of the thigh are in many cases relevant to pelvic anatomy. For example, the iliopsoas muscles leave the pelvis beneath the inguinal ligament with accompanying nerves to enter the thigh. The sartorius muscle is detached from the anterior superior iliac spine in radical vulvectomy surgery and transposed to cover the exposed femoral vessels. The gracilis muscle is utilized for pelvic reconstructive surgery as a myocutaneous graft. In addition to the muscles mentioned earlier, the gynecologist should be familiar with the fascia lata, tensor fascia lata muscle, rectus femoris, vastus lateralis, vastus medialis, pectineus, and adductor longus muscles (Figs. 1–14 and 1–15A and B). The muscles and fascia of the abdominal wall are discussed in detail in Chapter 7. However, the schema of the external oblique, internal oblique, rectus abdominis, and transversus abdominis muscles, and inguinal ligament are convenient to view in a single picture (Fig. 1–16). The inferior epigastric vessels are identified crossing the transversus abdominis fascia from their origin in the external iliac vessels. In this drawing, the left rectus abdominis muscle has been divided and the lower muscle belly has been reflected downward (caudal) to show the details of the inferior epigastric vessels, which lie on the post sheath of the rectus abdominis muscle and the transversus fascia. The triangle formed by the inferior epigastric vessels, the inguinal ligament, and the lateral border of the rectus is Hesselbach’s triangle (Fig. 1–17). Indirect inguinal hernias most commonly develop here (Hesselbach’s triangle). When the lower abdomen is opened, the peritoneal cavity is seen to be filled with intestines. A fat pad, the greater omentum, which is attached cranially to the greater curvature of the stomach and the transverse colon, hangs like an apron over the small and large intestines. Lifting the omentum reveals the large intestine on the periphery surrounding coils of small bowel. The large bowel is anchored normally to the parietal peritoneum along the right and left gutters (Fig. 1–18). The pelvic colon, or sigmoid colon, is a mobile intraperitoneal structure that is suspended by a mesocolon. The pelvic colon ranges from 5 to 35 inches in length and usually lies under the ileum. The rectum is 5 to 6 inches in length. It begins at the third sacral vertebra and hugs the curve of the sacrum, terminating just beyond the end of the coccyx. The rectum is covered only partially with peritoneum, with its upper third having peritoneal covering on the front and sides and the lower two thirds lying largely retroperitoneal (middle third has peritoneum in front only). The large bowel consists of cecum, ascending colon, transverse colon, descending colon, sigmoid colon, rectum, and anus. The blood supply to the large intestine emanates from the superior mesenteric artery (right colon and transverse colon) and the inferior mesenteric artery (left flexure, left colon sigmoid colon, upper two thirds of rectum), as well as the internal pudendal artery (anus and lower rectum). The venous drainage is to the hypogastric veins to a smaller extent and to the splenic, or portal, vein to a greater extent (Fig. 1–19). FIGURE 1–14 Muscles of the thigh are shown, together with their relationships to the saphenous vein, femoral vessels, and femoral nerve. Note that the saphenous vein lies in the fat (dissected away) overlying the adductor longus muscle. The femoral vein is directly superficial to the pectineus muscle. The femoral artery and nerve lie on the iliopsoas muscle(s). FIGURE 1–15 A. On the cadaver’s right side, the sartorius muscle has been removed, as have the rectus femoris and the vasti. Similarly, the tensor fasciae latae muscle, together with the fascia lata, has been removed to expose the course of the nerves and vessels, as well as the deeper muscles. B. On the cadaver’s left side, the obturator externus muscle, which covers the obturator membrane and foramen, is visible. Note the relationship of the latter to the pectineus muscle and the femoral vessels. Note that the adductor longus has been removed. On the right side, the adductor longus and pectineus muscles have been divided. FIGURE 1–16 The anterior abdominal wall has been dissected deeply on the patient’s left (viewer’s right) and more superficially on the right. The anterior rectus sheath and the aponeurosis of the external oblique muscle are prominent on the right. On the left, the external oblique has been cut and largely removed. The internal oblique and transversus abdominis muscles are exposed. Note the direction of the external and internal oblique, and of the transversus fibers. The anterior rectus sheath has been opened on the left side, allowing the entire left rectus abdominis muscle to be viewed. The anterior sheath of the rectus is derived only from the fascia of the external and internal obliques below the umbilicus. At this location, the posterior sheath is derived solely from the transversus abdominis muscle. FIGURE 1–17 The inferior epigastric vessels are important landmarks on the anterior abdominal wall, particularly because of their risk for injury during laparoscopic trocar entry. The artery arises from the lower medial aspect of the external iliac artery. The vein flows into the external iliac vein just cranial to the inguinal ligament. The femoral nerve emerges from within the substance of the psoas major muscle to be exposed directly under the tough inguinal ligament. This view shows the upper portion of the adductor longus, as well as the pectineus muscle. The latter overlies the obturator foramen (canal) and the obturator externus muscle, through which penetrate the obturator nerve plus the obturator vessels (not shown). Note also that the saphenous and femoral veins cross above the pectineus muscle. FIGURE 1–18 The transversus fascia, which is bound to the anterior parietal peritoneum, is cut and retracted, exposing the greater omentum (inset). When the greater omentum itself is retracted cranially, the underlying large and small intestines dominate the abdominal cavity. FIGURE 1–19 The blood supply to the right colon emanates from the superior mesenteric vessels. The inferior mesenteric vessels supply the left colon and sigmoid colon. The rectum receives blood from the inferior mesenteric vessels, as well as from branches of the hypogastric vessels. The inferior rectal vessels are branches and tributaries of the internal pudendal vessels. The transverse colon receives dual supply and drainage from superior and inferior mesenteric arteries and veins. The small intestine measures approximately 20 feet in length. The shortest portion of the small bowel is the duodenum (10 inches), which is closely related to the stomach at its first part and to the jejunum in its fourth part. The major portion of the small intestine consists of jejunum and ileum. The jejunum and ileum are totally surrounded by visceral peritoneum and are anchored to the posterior abdominal wall by a mesentery. The root of the mesentery is 6 to 8 inches in length and extends obliquely from the duodenojenunal flexure to the right colon. The small intestine itself extends from the ligament of Treitz to the ileocecal valve (Fig. 1–20). The superior mesenteric artery supplies the small intestine by a series of arcades. Venous drainage occurs via the superior mesenteric vein to the portal vein (Fig. 1–21). The ileum should be carefully examined 2 to 3 feet before the ileocolic junction for the presence of a finger-like projection called Meckel’s diverticulum. This is located on the antimesenteric border. When the small and large bowels are retracted, the uterus, adnexa, and urinary bladder are brought into view (Fig. 1–22). The posterior and lateral parietal peritonei are clearly and similarly viewed but cover the underlying retroperitoneal structures. The peritoneum is incised over the psoas major muscle. The muscle (which may include the psoas minor) is exposed, and the genitofemoral nerve is identified. At the medial margin of the pelvic portion of the psoas muscle is the external iliac artery. Beneath the artery is the larger external iliac vein. The external iliac artery is dissected retrograde and cephalad for identification of the common iliac artery and vein. The latter are marked by the crossover of ovarian vessels coupled with the ureter (Figs. 1–22 and 1–23). The common iliac bifurcation should be identified. The common iliac vein is seen to lie in the crotch formed by the bifurcation of the internal and external iliac arteries. Continuing in a cephalad direction, the common iliac arteries are dissected to their origin at the bifurcation of the abdominal aorta
Introduction to Pelvic
Anatomy 1
![]()
Stay updated, free articles. Join our Telegram channel


Full access? Get Clinical Tree


