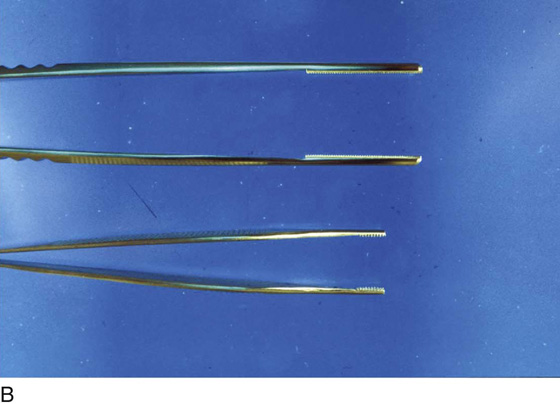
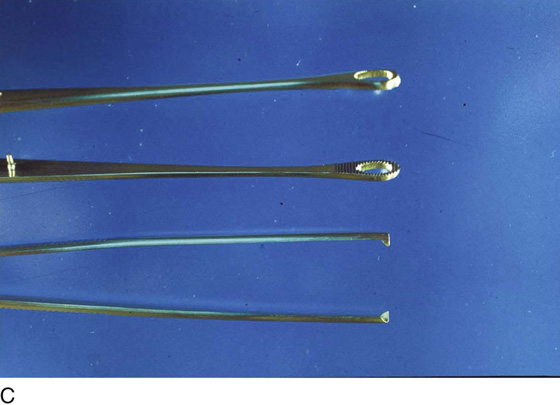
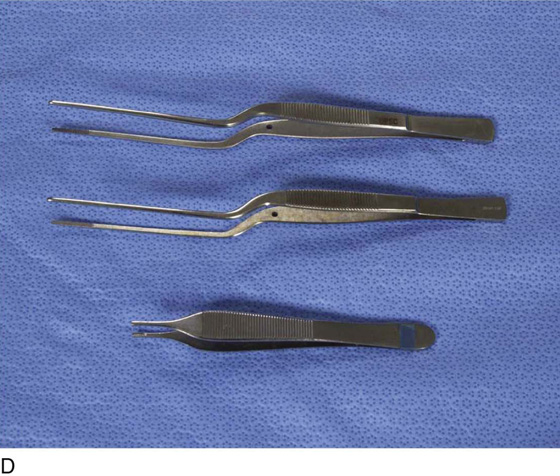
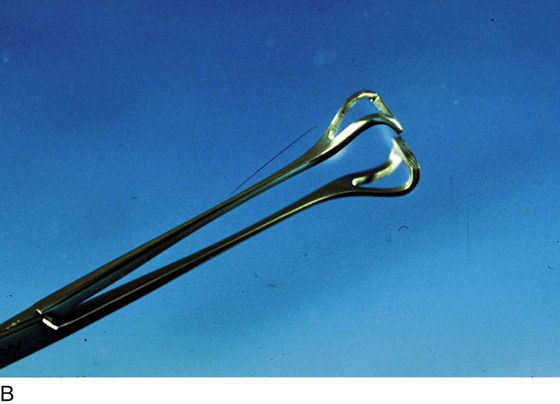
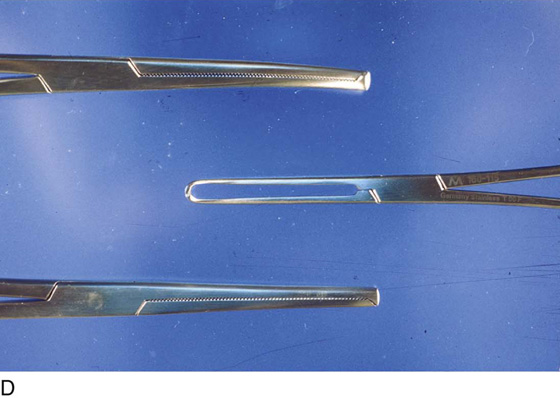
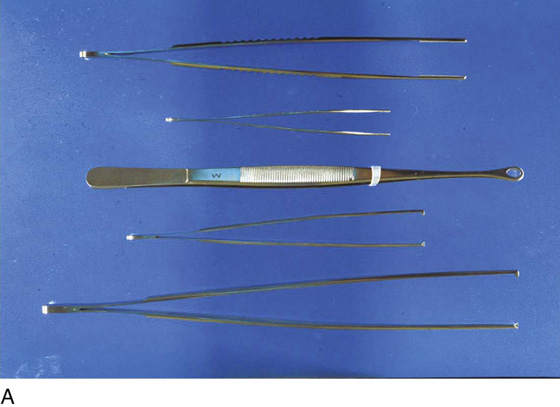
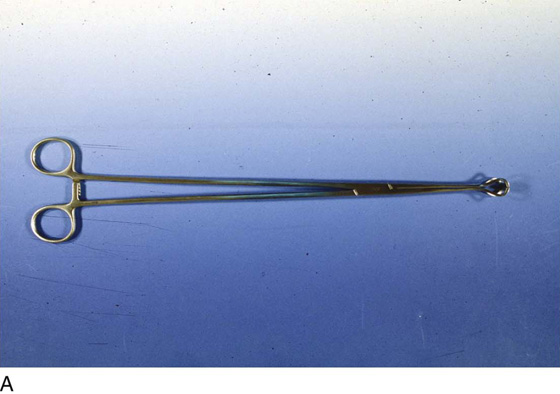
CHAPTER 3 A surgeon’s tools are analogous to those of a carpenter, a mechanic, a research chemist, or an atomic physicist. High-quality instruments are required for the performance of precise and excellent surgery. Although a fine surgeon may overcome the deficits of inferior instruments, the real and potential difficulties presented by using second-rate tools make doing first-rate surgery harder. Good instruments coupled with good surgeons yield the best outcomes. Throughout this book, reference is made to various instruments utilized in the performance of specific operations. For convenience, this section will codify the panoply of instruments commonly used in gynecologic surgery. A number of forceps are available. Atraumatic forceps include the Adson and DeBakey instruments. For lymph node and fat dissection, for example, obturator fossa dissection, ring forceps are quite acceptable. Rat-tooth forceps are excellent for traction and for holding tissue securely; however, they may traumatize skin and other delicate tissues. Adson-Brown forceps are the best instruments for grasping skin edges during closure procedures (Fig. 3–1A–C). For fine work deep in the pelvis, for example, dissecting around the ureter or iliac vessels, the author prefers a bayonet forceps equipped with a brown-toothed tip (Fig. 3–1D, E). Clamps may be subdivided into grasping and traction clamps, which include Allis and Ochsner clamps. Grasping clamps are relatively atraumatic, whereas traction clamps are best suited to specimens that will be excised or otherwise removed. Allis clamps are frequently required in vaginal and abdominal surgery. Babcock clamps are atraumatic instruments useful for grasping delicate structures, such as the oviducts, utero-ovarian ligaments, and other fragile tubular structures (Fig. 3–2A, B). Ochsner clamps, for example, may be applied to the cervix for traction during vaginal hysterectomy or on skin scars that are going to be cut out (Fig. 3–2C, D). Dissecting or hemostatic clamps include standard and long tonsil clamps (Fig. 3–3A, B). These are excellent for fine dissection and for clamping bleeding vessels deep within the pelvis, particularly in strategic locations. The tips of these clamps are tapered and angled. One variety, the right-angle clamp, has a 90° angle (Fig. 3–3C). This is the instrument of choice for isolating large arteries from underlying veins, as occurs during hypogastric artery ligation. Hemostatic clamps may be straight or curved. Mosquito clamps and the larger Kelly clamps are most commonly used to secure bleeding vessels. Additionally, the fine mosquito clamps may also be used as dissecting tools (Fig. 3–4A, B). Large vascular pedicle clamps used for hysterectomy or radical hysterectomy should incorporate powerful, atraumatic jaws, a variety of curvatures, and suitable length to facilitate securing these large pedicles. These characteristics are exemplified by the Zeppelin clamps (Fig. 3–5A–C). Haney clamps of the straight and curved variety are the most common pedicle clamps used in the performance of vaginal hysterectomy (Fig. 3–5D). Surgical scissors may be divided into fine dissecting instruments and heavy-duty mass-cutting devices. The first category includes Metzenbaum and Stevens scissors. The former are superior for dissection, whereas the latter are the superlative cutting tools (Fig. 3–6A, B). Large pedicles, vaginal cuffs, and ligaments are best cut with Mayo or Jorgenson scissors (Fig. 3–7A, B). Of course, the sharpest mechanical cutting tool is the scalpel. A variety of blade shapes are available for different applications. Scalpel handles may be a standard 6-inch length or an elongated 9- to 10-inch length (Fig. 3–8). During contemporary abdominal surgery, a self-retaining retractor is essential. Several types are available, ranging from the frame type (Bookwalter and Kirschner) to the spreading type (O’Sullivan-O’Connor). The modern frame retractor has the advantage of remote location, that is, location outside of the abdominal cavity. Its varied blades may be placed within the abdomen and interchanged when necessary without compromising exposure or completely removing the retractor (Fig. 3–9A, B). The O’Sullivan-O’Connor retractor and the Balfour retractor are the most commonly used devices for pelvic surgery. The O’Sullivan-O’Connor retractor is easy to use and has a sufficient variety of blades to satisfy most clinical conditions. This retractor is equally suitable for transverse and vertical incisions (Fig. 3–10A, B). The Balfour retractor is also a mainstay abdominal retractor in gynecologic and obstetric surgery. This device may be alternatively fitted with standard or deep lateral retractor pieces (Fig. 3–10C, D). FIGURE 3–1 A. Five surgical forceps are shown. From the top: DeBakey, Adson-Brown, ring, rat-tooth, standard (6-inch), and medium (10-inch) tissue forceps. B. Close-up view of the atraumatic DeBakey (top) and Adson-Brown forceps (bottom). C. Close-up view of the ring forceps, which are ideal for clearing fatty tissue from the obturator fossa and between large vessels. Below is the grasping end of rat-tooth tissue forceps. D. Bayonet forceps (top and center) and Adson forceps (bottom) are ideal for fine tissue handling. E. Another view of the forceps shown in Figure 3–1D. FIGURE 3–2 A. The Babcock clamp, which ranges in length from 8 to 14 inches, is an atraumatic grasping instrument ideal for placing traction on tubular structures while not crushing the tissue. B. Close-up of the shaft and terminus of the Babcock clamp. C. The three clamps illustrated here are curved Ochsner (top), Allis (center), and straight Ochsner clamps (bottom). D. Close-up view of Figure 3–2C. Note the toothed jaws of the Ochsner clamps (top), which grasps very securely but is rather rough on the tissue. In contrast, the Allis clamp (center
Instrumentation
Forceps
Clamps
Scissors
Knives
Retractors


![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


