This chapter includes discussions of selected tick-borne, zoonotic, and parasitic infections.
TICK-BORNE AND ZOONOTIC INFECTIONS
Rocky Mountain Spotted Fever
Rocky Mountain spotted fever (RMSF), caused by Rickettsia rickettsii, is the most prevalent rickettsial disease in the United States. It is most common in the southeastern and south central regions of the United States. Ticks, wild animals, and dogs serve as reservoirs of infection, and a tick bite is the usual mode of transmission. Children younger than 15 years account for two thirds of cases, and the disease is most common in spring and summer.
R. rickettsii causes a vasculitis that clinically manifests with fever, headache, rash, myalgias, and changes in mental status. The rash can be maculopapular or petechial and usually begins peripherally on the wrist and ankle and spreads centripetally. The palms and soles are commonly involved. Leukopenia, thrombocytopenia, anemia, elevated levels of aminotransferases and bilirubin, and hyponatremia are common laboratory findings.
A definitive diagnosis often cannot be made until the second week of illness because serologic assays are not sensitive early in the course of the disease. Fluorescent or peroxidase-tagged antibody tests of specimens from skin lesions can provide a rapid and highly specific diagnosis.
The differential diagnosis of RMSF includes:
Meningococcemia
Ehrlichiosis
Atypical measles
Enteroviral infection
Henoch-Schönlein purpura
Leptospirosis
Because the diagnosis often cannot be confirmed until the second week of the illness, a high index of suspicion and presumptive therapy is required. The institution of antimicrobial therapy within 6 days of the onset of illness is associated with low mortality. Doxycycline is the treatment of choice for children of any age; although the tetracyclines are generally contraindicated in children <8 years of age, doxycycline is recommended for the treatment of RMSF, regardless of age, given the effectiveness of this therapy, the low adverse effect profile even in young children, and the lack of effective alternative antimicrobials. Severe morbidity and mortality from cardiac failure, vascular collapse, and renal failure can occur and are usually related to a delayed diagnosis.
Ehrlichiosis
Human monocytic ehrlichiosis is caused by Ehrlichia chaffeensis; human granulocytic ehrlichiosis is caused by Anaplasma (formerly Ehrlichia) phagocytophila and Ehrlichia ewingii. Both forms of ehrlichiosis are transmitted by a tick bite; known reservoirs include the white-tailed deer and white-footed mouse. E. chaffeensis infections occur mainly in the southeastern and south central regions of the United States; most cases of human granulocytic ehrlichiosis have occurred in Wisconsin, Minnesota, Connecticut, and New York. The infections generally develop in spring and summer, and adults appear to be at greatest risk, although infection with E. chaffeensis is common in children. Immunocompromised individuals appear to be at greatest risk for severe infection.
The clinical features of the two types of human Ehrlichia infection are similar and also quite similar to the clinical features of RMSF. Rash is less common in ehrlichiosis, whereas anemia, leukopenia, and thrombocytopenia are more common in ehrlichiosis than in RMSF.
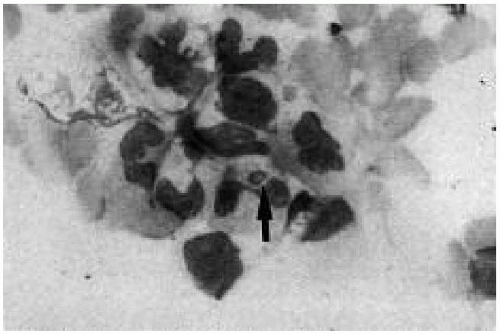
The identification of intraleukocytic inclusions (morulae) in peripheral blood monocytes (Fig. 50.1) or granulocytes and acute and convalescent serologic titers are used to confirm the diagnosis.
Doxycycline is the drug of choice for the treatment of Ehrlichiosis in children of any age.
Figure 50.1 Peripheral blood smear showing an intraleukocytic inclusion (morula), characteristic of Ehrlichia infection. (See color insert.)
Tularemia
The etiologic agent of tularemia is Francisella tularensis, a small gram-negative coccobacillus. Important reservoirs of infection include rabbits, hares, and ticks. The most important route of transmission is a tick bite, but transmission can also result from direct contact with infected animals, aerosolization of the organism, or ingestion of contaminated water or meat. Infection is most common in the central states of Arkansas, Missouri, Tennessee, and Texas between the months of April and September.
The ulceroglandular form is the most common form of infection and is characterized by fever, regional lymphadenopathy, and skin lesions, usually an ulcer or papule at the site of inoculation. Pharyngitis, myalgias, vomiting, and hepatosplenomegaly may be present. Other forms of disease may also occur (glandular, pneumonic, oculoglandular), depending on the portal of entry of the organism.
A history of exposure to the organism (tick bite, close contact with rabbits) along with the characteristic clinical picture should lead the examiner to suspect tularemia. Serologic testing may be helpful diagnostically.
Streptomycin is the drug of choice, with gentamicin an effective alternative.
Leptospirosis
Leptospira organisms are spirochetes found in many wild and domestic mammals, including dogs, rats, and livestock. Transmission to humans results from contact with water and soil infected with the organism or from direct contact with infected animals. Contaminated farm ponds and animal slaughterhouses are settings in which transmission occurs.
Subclinical infection is most common, but clinical illness can manifest in either an anicteric (milder) or icteric (severe) form. Anicteric disease accounts for 90% of cases and presents with an abrupt onset of fever, headache, myalgia, and subconjunctival suffusion; a second phase of disease often follows, characterized by fever, rash, uveitis, and meningitis. The organism can be recovered from the blood and spinal fluid in the first phase of illness, and from the urine in the second phase. Icteric leptospirosis, also known as Weil syndrome, occurs in 10% of cases and is characterized by severe illness with liver and renal failure, hemorrhage, and myocarditis.
Special laboratory techniques are required to recover the organism. Serologic assays are utilized in confirming the diagnosis.
Most cases are self-limited. Patients with severe disease requiring hospitalization should be treated with intravenous penicillin. Amoxicillin and doxycycline (for children 8 years of age and older) are alternative therapies for patients with mild disease.
Lyme Disease
Borrelia burgdorferi is the etiologic agent of Lyme disease. Infected ticks serve as the vectors of transmission. Reservoirs include the white-footed mouse, birds, lizards, and deer. In the United States, most cases of Lyme disease are seen in the northeastern states, upper Midwest (Minnesota and Wisconsin), and northern California. Most cases occur between April and October.
The clinical manifestations can be categorized as:
Early localized disease, occurring 3 days to 4 weeks after a tick bite
Early disseminated disease, developing 4 weeks to 8 weeks after infection
Late disease, occurring 2 months to several years after infection
In early localized disease, erythema migrans(Figs. 50.2, 50.3) develops at the site of the tick bite, which may or may not be recalled. Erythema migrans begins as an erythematous papule that expands to become an annular lesion measuring 3 to 15 cm, often with central clearing but occasionally with a vesicular center. Multiple small lesions may also be present. Biopsy of the lesion with special culture media often reveals the organism. The lesion is frequently confused with ringworm, a spider bite, or nummular eczema. Nonspecific symptoms, such as fever, malaise, and arthralgias, may be present at this stage. Antibodies to B. burgdorferi are consistently absent at this stage of infection and remain so in persons who receive treatment at this stage. Although most untreated persons recover completely without further disease, late manifestations of Lyme disease develop in approximately 20% of untreated cases.
Figure 50.2 Erythema migrans in an adolescent with Lyme disease. Note the annular lesion with central clearing, characteristic of the rash. (See color insert.)
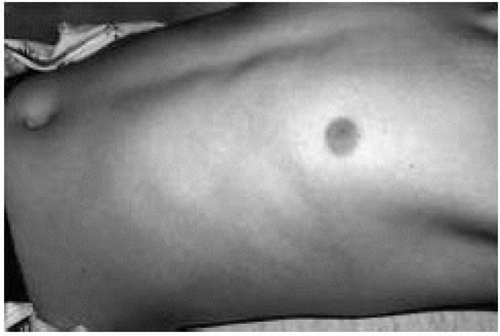
Figure 50.3 Annular lesion of erythema migrans in the axilla of a 12-year-old boy who presented with fever and this rash following a camping trip to eastern Pennsylvania. Note the presence of a small vesicle at the center of the lesion. (See color insert.)
Features of early disseminated disease include:
Multiple circular lesions
Flu-like illness
Neuritis (seventh cranial nerve palsy)
Aseptic meningitis
Carditis
Meningitis develops in a small percentage of untreated persons and manifests as headache, photophobia, and neck stiffness. The CSF fluid is aseptic with a lymphocytic pleocytosis, mildly elevated protein level, and normal glucose level. The diagnosis can be confirmed by demonstrating the intrathecal production of specific antibodies. Seventh cranial nerve palsy is more common than meningitis and is selflimited. Treatment does not alter the course of the neuritis but prevents late complications of infection. Carditis is quite uncommon, occurring in <5% of infected persons, and usually manifests as a transient alternating heart block.
Lyme arthritis is by far the most frequent manifestation of late disease. Lyme arthritis is characterized by involvement of the knee in >90% of cases and may be monoarticular or pauciarticular. The course may be chronic and intermittently flaring. Encephalopathy and polyneuropathies occur very rarely.
Early in the course of infection the diagnosis can be made clinically based on the appearance of the characteristic rash in a patient from an area in which Lyme disease is endemic. Routine serologic tests are not indicated in children with typical symptoms. Serologic tests can be helpful in diagnosing later stages of Lyme disease when the appropriate clinical features are present. This should be accomplished using an enzyme immunoassay and confirmed by Western immunoblot testing. When serologic tests are considered, only reference laboratories should be utilized. Serologic studies are not recommended for children with nonspecific symptoms whose probability of having Lyme disease is low, because these tests can be nonspecific.
The treatment recommendations for children with Lyme disease are summarized in Table 50.1. When children are treated according to these recommendations, the outcome is excellent. Prolonged (beyond the periods specified in Table 50.1) or repeated courses of antimicrobial therapy for Lyme disease are not indicated. Chemoprophylaxis following a tick bite, even for people living in areas of endemicity, is not routinely recommended.
Rat Bite Fever
Rat bite fever is caused by Streptobacillus moniliformis (more common in the United States) or Spirillum minus, which live in the upper respiratory tract of rodents. Rats are the most common source of infection, but other rodents, including mice, squirrels, and gerbils, can serve as additional reservoirs.
Symptoms of rat bite fever include abrupt onset of fever, myalgias, emesis, and headache. A maculopapular or petechial rash on the extremities is common; however, the bite site commonly heals quickly and is no longer visible at presentation. Migratory polyarthritis occurs in about 50% of patients, whereas pneumonia, endocarditis, and meningitis are rare. Without specific treatment, a relapsing course of symptoms can occur for several weeks. The diagnosis requires clinical suspicion. Recovery of S. moniliformis from the blood requires enriched culture media and prolonged incubation for up to 3 weeks.
TABLE 50.1 TREATMENT OF LYME DISEASE IN CHILDREN
Stage of Illness
Treatment Recommendations
Early localized disease
≧8 years old
Doxycycline 100 mg orally twice a day for 14-21 days
All ages
Amoxicillin 50 mg/kg/day (maximum 1.5 g/day) for 14-21 days, OR
Cefuroxime 30 mg/kg/day (maximum 1000 mg/day) for 14-21 days
Early disseminated and late disease
Multiple erythema migrans
Same oral regimen as for early localized disease but for 21 days
Meningitis
Ceftriaxone 75-100 mg/kg (maximum 2 g/day) IV for 14-28 days, or Penicillin G 300,000 U/kg/day (maximum 20 million U/day) IV for 14-28 days
Isolated facial palsy
Same oral regimen as for early localized disease but for 21-28 days
Carditis
Same as for meningitis
Arthritis
Same oral regimen as for early localized disease but for 28 days
Persistent or recurrent arthritis
Ceftriaxone 75 mg/kg IV or IM for 14-21 days, or Penicillin G 300,000 U/kg/day IV for 14-28 days, or same oral regimen as for early disease IM, intramuscular; IV, intravenous.
Only gold members can continue reading. Log In or Register to continue