Fig. 18.1
Pathophysiology of infantile hypertrophic pyloric stenosis
Signs and Symptoms
There is progressively projectile and non-bile-stained vomiting. The child remains hungry and takes food immediately after vomiting.
Poor weight gain and malnutrition (Fig. 18.2).

Fig. 18.2
a and b Clinical photograph of patients with infantile hypertrophic pyloric stenosis with poor weight gain, malnutrition, dehydration, and epigastric fullness
Ninety-five percent have a palpable pyloric mass (olive sign) which is felt in the right upper abdomen, especially after vomiting and during a test feed.
May be dehydrated.
Visible peristalsis in the epigastrium travelling from left to right (Fig. 18.3).
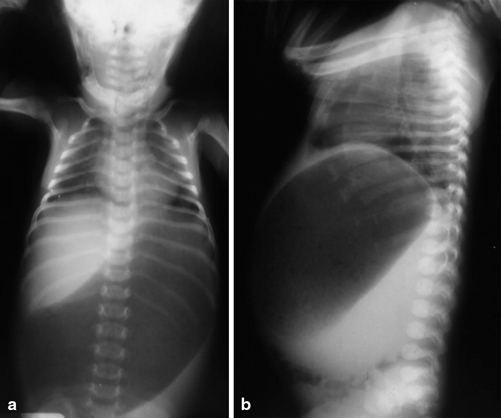
Fig. 18.3
a and b Abdominal X-ray showing markedly dilated stomach
Indirect hyperbilirubinemia may be seen in 1–2 % of affected infants.
Diagnosis
Diagnosis is via a careful history and physical examination, often supplemented by radiographic studies.
Abdominal radiographs are not necessary and may show a fluid-filled or air-distended stomach, suggesting the presence of gastric outlet obstruction. A markedly dilated stomach with exaggerated incisura (caterpillar sign) may be seen (Figs. 18.3 and 18.4).
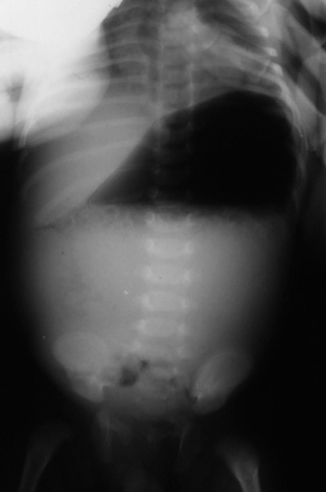
Fig. 18.4
Erect abdominal X-ray showing dilated stomach with air fluid level in a patient with infantile hypertrophic pyloric stenosis. Note the scanty gas in the distal bowel
Current imaging techniques , particularly ultrasonography, are noninvasive and accurate for identification of infantile hypertrophic pyloric stenosis . Ultrasonography is the method of choice for the diagnosis of hypertrophic pyloric stenosis, because it has a sensitivity and specificity of almost 100 %.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


