We read with interest the recent article by Roberge et al on an interesting approach to a uterine closure that influences the healing of uterine scars. They demonstrated that the double-layer uterine closure with a first unlocked layer that excludes the decidua, compared with locked single-layer closure that includes the decidua, is associated with a greater residual myometrial thickness (RMT) and healing ratio, which suggests that this technique is associated with better healing of the uterine scar. However, we would like to discuss some disagreements with the authors’ comments about the implications of myometrial closure, including the decidua to the RMT and healing ratio.
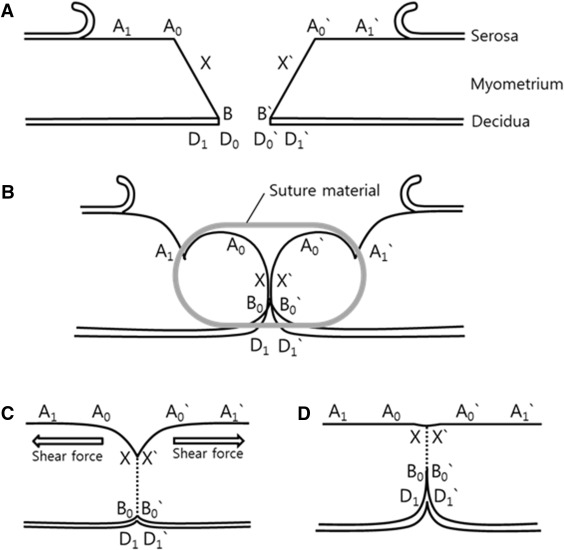
We believe that the main causative factor of the RMT is the coaptation ratio of incised myometrium (BX / A 0 B; Figure , A). When a single layer with a locking suture is used to penetrate the full thickness of myometrium and the decidua, the 2 points of A 0 and A 0 ’ barely join each other, even after the absorption of suture materials ( Figure , B, C, and D), because the uterus that delivered the baby is a dynamically contracting, globular, and muscular organ. Moreover, the presence and length of the uncoaptated portion (X-A 0 ) are the predominant factors that influence the different degree of RMT. Therefore, the surgeon should aim to minimize the length of the line “D 0 -D 1 ” and not exclude the decidua itself. This would minimize the potential adverse effect that is associated with the inversion of the decidua (such as adenomyosis) or influence RMT and prevent the postoperative endometrial defect of exposure of the myometrium to the endometrial cavity.