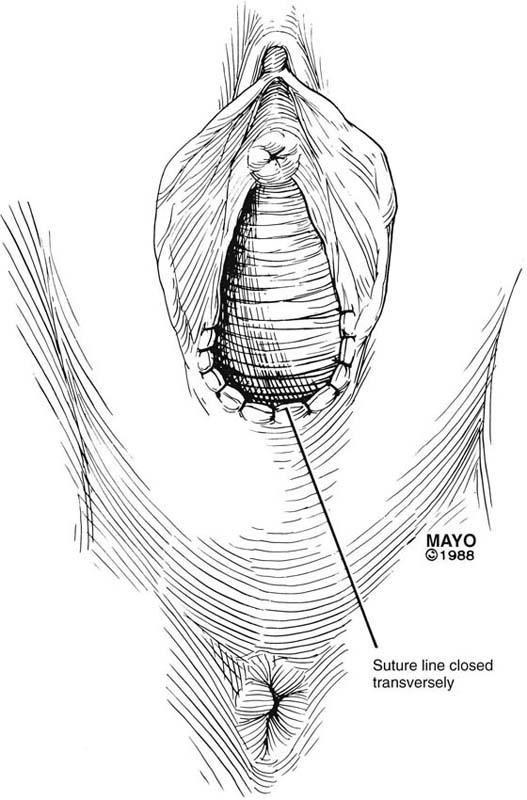
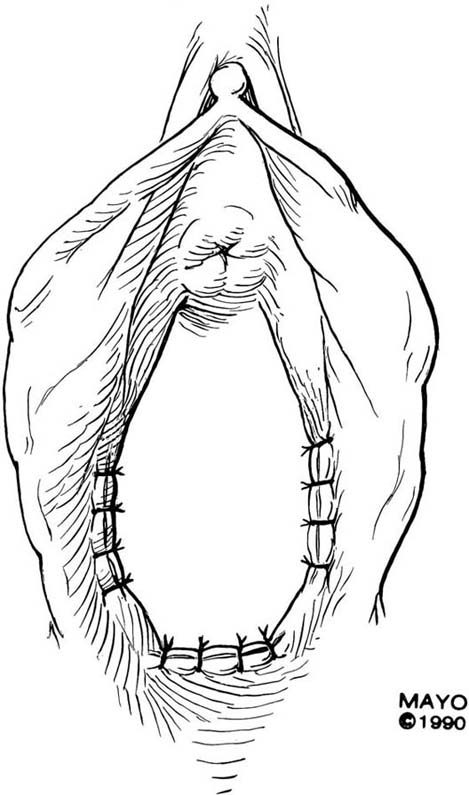
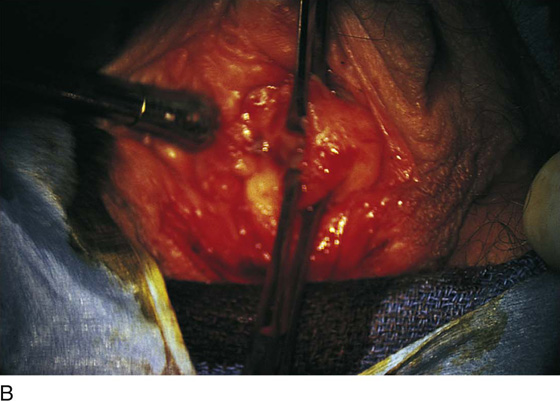
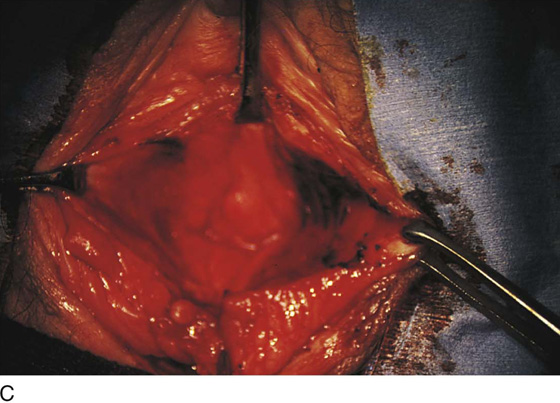
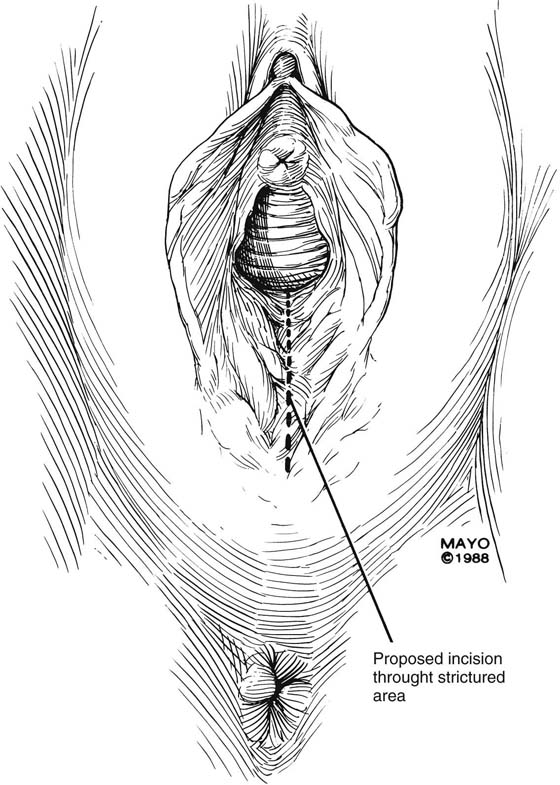
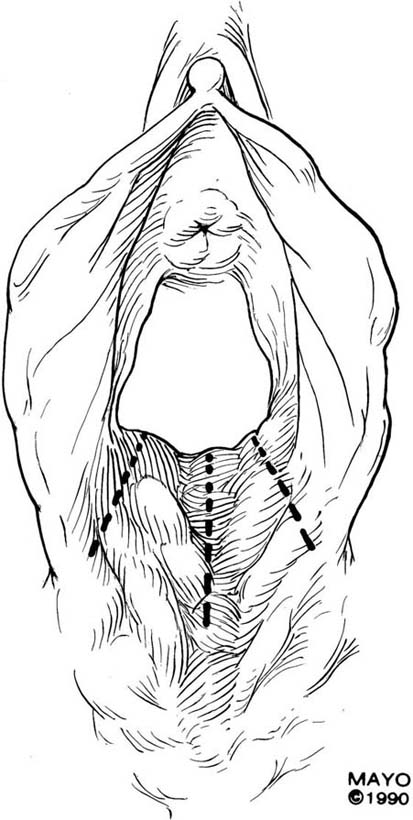
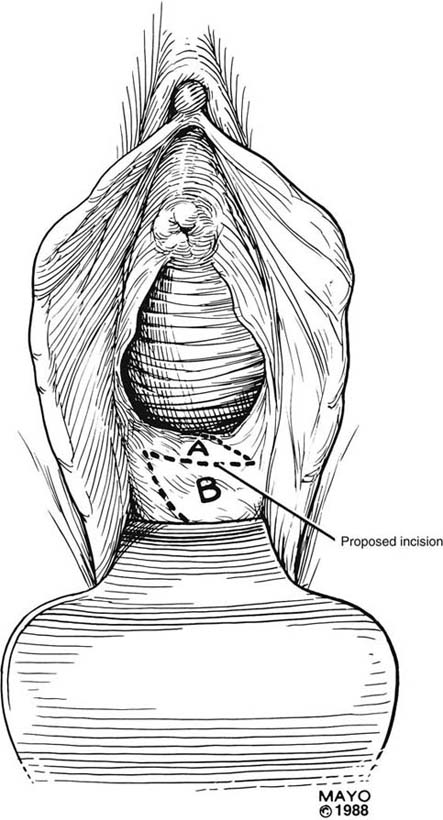
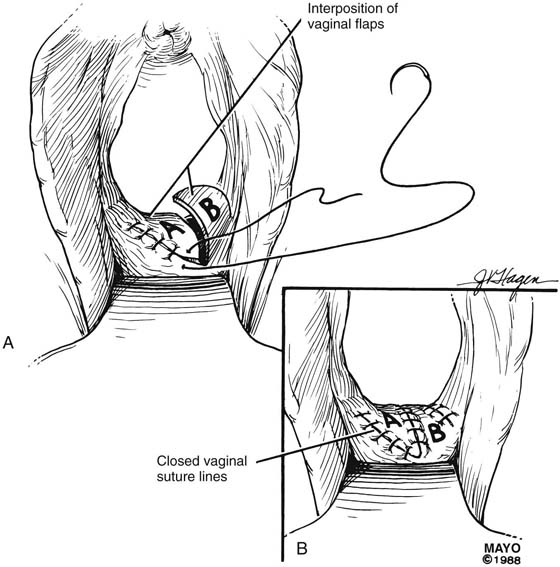
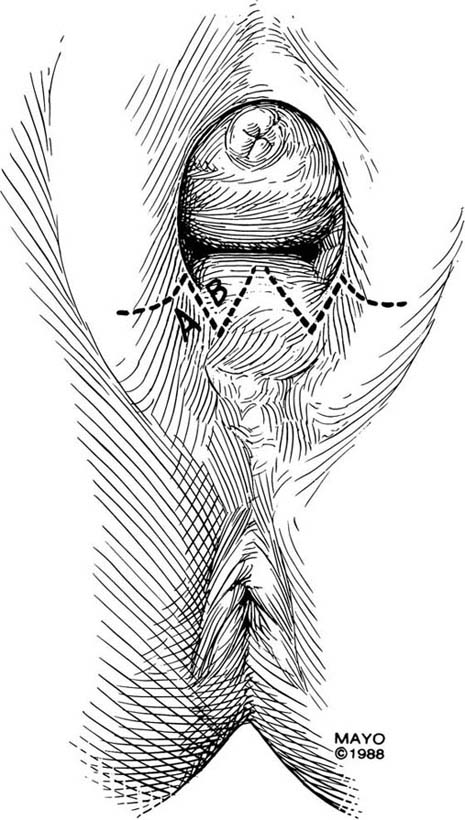
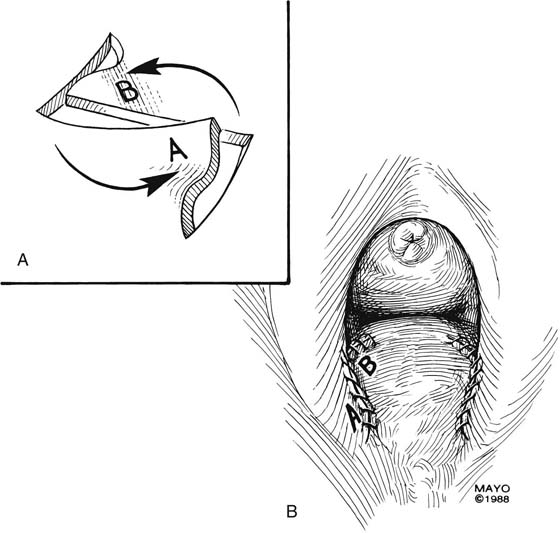
CHAPTER 62 John B. Gebhart Vaginal stricture may occur secondary to inflammatory conditions of the vagina, vaginal surgery, episiotomy repair, or radiotherapy. The surgical approach to the stenosis depends on its anatomic location, underlying cause, and severity. For introital or vaginal stenosis, the procedure can treat both upper and lower vaginal strictures or can correct lower vaginal strictures specifically. Operations that correct upper and lower vaginal strictures include incision of the vaginal constriction ring or ridge, vaginal advancement, Z-plasty, free skin graft, perineal flaps, and abdominal flaps. Restenosis risk is high after these interventions; therefore, postoperative care must include rigid dilation that is initiated immediately in the postoperative period. The simplest approach to a vaginal constriction is a midline incision of the contracting scar or ridge. The midline incision is made, and the vaginal mucosa is mobilized from the underlying scar (Fig. 62–1). Excessive scar tissue may be excised completely to increase the vaginal or introital diameter. When hemostasis is achieved, the wound may be left to heal by secondary intention, or the vaginal tissue may be undermined and advanced and the incision closed transversely in a tension-free manner (Fig. 62–2). When a single midline incision with transverse closure is inadequate, numerous vertical incisions may be made (Fig. 62–3). Separate vertical incisions are closed transversely—after mobilization of surrounding vaginal tissues—to obtain sufficient introital or vaginal diameter (Fig. 62–4). Figure 62–5A shows a midvaginal constriction ring after an overzealous anterior and posterior colporrhaphy. The stenotic site was initially enlarged with the use of Hegar dilators passed from the lower vaginal segment into the upper segment. When the vagina was dilated to at least 10 mm, bilateral longitudinal incisions were made in the lateral aspect of the stenotic site and were taken along the vaginal axis (Fig. 62–5B). The tight fibrous band was completely excised, and the dissection continued until loose connective tissue was encountered in the ischiorectal space (Fig. 62–5C). Some surgeons prefer to leave the space open; others prefer to close it transversely and perpendicular to the original incision, using interrupted, 3-0 absorbable sutures. The Z-plasty technique involves transplantation of two interdigitating triangular flaps. The orientation of the Z may be vertical or transverse, depending on the stricture. The degree of stenosis determines the incision length of the flap arms and the flap angles. Typically, the flaps are 2 cm long and at 60° angles. Additional diameter is gained by increasing the angle. The midpoint, or the site of the most severe contracture, is identified, and a transverse incision is made (this incision becomes the common limb of the Z-plasty). The upper arm of the Z is extended into the vagina; the lower arm is extended toward the perineum (Fig. 62–6). Scar tissue, if present, may be excised, and the transposed flaps are reapproximated with interrupted, 3-0 or 4-0 absorbable sutures (Fig. 62–7). Introital stricture may be amenable to a transverse Z-plasty. This technique results in the absence of a midline suture line. Duplication of the flaps at the 4- and 8-o’clock positions of the introitus results in an increase in introital diameter (Fig. 62–8). Care must be taken to approximate the apices of the incisions and thereby to gain maximum transverse diameter. “Dog ears” should be trimmed and absorbable sutures used to produce a smooth approximation of tissues (Fig. 62–9). FIGURE 62–1 A midline incision is made and the vaginal mucosa is widely mobilized, excising the underlying scar tissue as needed. (Adapted from Lee RA: Atlas of Gynecologic Surgery. Philadelphia, WB Saunders, ©1992. Used with permission of Mayo Foundation for Medical Education and Research.) FIGURE 62–2 To increase vaginal diameter, the initial vertical incision is closed in a transverse manner. (Adapted from Lee RA: Atlas of Gynecologic Surgery. Philadelphia, WB Saunders, ©1992. Used with permission of Mayo Foundation for Medical Education and Research.) FIGURE 62–3 In cases of broader areas of scarring and stenosis, numerous vertical incisions may be used. The surrounding tissues are mobilized, and excessive scar tissue is excised. (Adapted from Lee RA: Atlas of Gynecologic Surgery. Philadelphia, WB Saunders, ©1992. Used with permission of Mayo Foundation for Medical Education and Research.) FIGURE 62–4 Numerous vertical incisions may be converted to multiple transverse closures, thereby increasing the diameter at the area of stricture. (Adapted from Lee RA: Atlas of Gynecologic Surgery. Philadelphia, WB Saunders, ©1992. Used with permission of Mayo Foundation for Medical Education and Research.) FIGURE 62–5 A. Midvaginal constriction ring that occurred after an overzealous anterior and posterior repair. The image shows the Hegar dilator in the small opening. B. Because the vagina was sufficient above this ring, bilateral relaxing incisions were performed to reopen the vagina. Allis clamps were used to grasp the ring in preparation for the incision. An incision was made at both 4 and 7 o’clock. C. The incisions were continued until the band was completely incised and loose areolar tissue was encountered. The incision was left open to heal by secondary intention. FIGURE 62–6 The midpoint of the scar is identified, and a transverse incision made. This incision site becomes the common arm of the Z-plasty. The upper arm of the Z is extended into the upper vagina; the lower arm of the Z is extended toward the perineum. The area of stricture determines the length and angle of the incisions. (Adapted from Lee RA: Atlas of Gynecologic Surgery. Philadelphia, WB Saunders, ©1992. Used with permission of Mayo Foundation for Medical Education and Research.) FIGURE 62–7 A. After mobilization, the scar tissue is excised and the flaps interposed. B. The transposed flaps are reapproximated in a tension-free manner with interrupted sutures. (Adapted from Lee RA: Atlas of Gynecologic Surgery. Philadelphia, WB Saunders, ©1992. Used with permission of Mayo Foundation for Medical Education and Research.) FIGURE 62–8 The Z-plasty may be made on either side of the introital opening, which results in a lateral incision closure and the absence of an incision in the midline. (Adapted from Lee RA: Atlas of Gynecologic Surgery. Philadelphia, WB Saunders, ©1992. Used with permission of Mayo Foundation for Medical Education and Research.) FIGURE 62–9 A. After the incisions are made and the tissues mobilized, the subcutaneous tissues are separately approximated. B. The overlying mucosa is closed with interrupted, 4-0 delayed absorbable suture. (Adapted from Lee RA: Atlas of Gynecologic Surgery. Philadelphia, WB Saunders, ©1992. Used with permission of Mayo Foundation for Medical Education and Research.)
Iatrogenic Vaginal Constriction
 Mickey M. Karram
Mickey M. Karram
Introduction
Incisions
Z-Plasty
Free Skin Grafts

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


