Hyperandrogenism
Katherine Ikard Stewart
Lisa Kolp
Androgens are necessary for normal ovarian and sexual function. They play an important role in cognition, bone health, muscle mass, body composition, mood, and energy. The obstetrician-gynecologist must have a strong knowledge base regarding the role androgens play in normal female physiology.
Androgens are precursors for estrogen synthesis.
Although controversial, it has been proposed that androgens may be necessary for normal sexual desire in women.
Androgens also affect skeletal homeostasis. They affect bone metabolism directly via androgen receptors expressed by osteocytes and indirectly via conversion of androgens to estrogen. Multiple studies have shown that women with low androgen concentrations have lower bone density and increased fracture risk.
ANDROGENS IN THE FEMALE
Androgens circulate in the body in various forms. Circulating androgens found in the blood of premenopausal women include testosterone, androstenedione, dehydroepiandrosterone (DHEA), DHEA sulfate (DHEA-S), and dihydrotestosterone (DHT). Androgens are produced by the adrenal glands and the ovary and arise from peripheral conversion.
Testosterone
Testosterone is the most potent androgenic hormone.
In women, nearly 25% of testosterone is secreted from the ovaries and 25% is from the adrenal glands. The remaining one half is produced from peripheral conversion of androstenedione to testosterone in the kidneys, liver, and adipose tissue.
Normal circulating concentrations range from 20 to 80 ng/dL.
Approximately 65% of testosterone in the circulation is bound to sex hormone-binding globulin (SHBG). Nineteen percent to 33% of testosterone is loosely bound to albumin. The remaining 1% of testosterone circulates in the free and active form (Fig. 41-1).
Testosterone levels decrease by 50% from ages 20 to 40 years. Less testosterone is secreted from the ovary with menopause, as the ovarian theca cells are less responsive to luteinizing hormone (LH). As menopause is entered, SHBG levels remain constant, yielding an even greater decrease in free testosterone. However, serum hormone concentrations of SHBG fall due to the lack of estrogen, finally resulting in an increase in bioavailable testosterone.
Androstenedione
Is a less potent androgen than testosterone but can produce significant androgenic effects when present in excess amounts
Is produced in equal amounts by the adrenal glands (50%) and the ovaries (50%)
Majority of androstenedione is converted to testosterone.
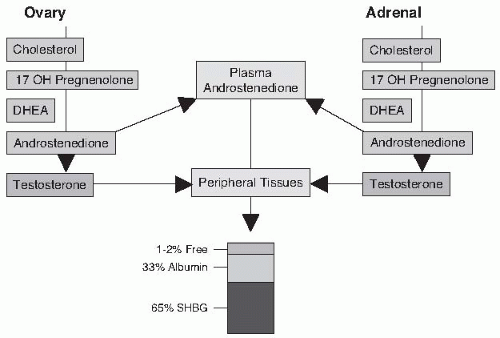
Figure 41-1. Endogenous production and secretion of testosterone in women. DHEA, dehydroepiandrosterone; SHBG, sex hormone-binding globulin.
Normal serum concentration ranges from 60 to 300 ng/dL, often with a 15% increase at midcycle. Androstenedione circulates in blood, bound to both SHBG and albumin.
Dehydroepiandrosterone and Dehydroepiandrosterone Sulfate
Androgen precursors, much less potent than testosterone, are produced predominantly by the adrenal glands, with some component of ovarian production and peripheral conversion.
DHEA is metabolized quickly, thus measurement of its serum concentration does not reflect adrenal gland activity. DHEA-S has a much longer half-life than DHEA, and measurement of its serum level is used to assess adrenal function.
Serum hormone concentrations of DHEA-S in women vary widely and depend on age (normal range of approximately 35-340 µg/dL depending on the lab).
Dihydrotestosterone
Testosterone is converted to DHT by 5-alpha reductase, an enzyme found in many androgen-sensitive tissues.
DHT is a very potent androgen primarily responsible for the androgenic effects on hair follicles.
Sex Hormone-Binding Globulins
Androgenicity is determined by free hormone concentrations. Thus, SHBG influences the hormonal state. Testosterone and insulin both decrease SHBG levels, whereas estrogen and thyroid hormone increase its levels.
Symptoms of hyperandrogenism may be seen in patients with a normal total testosterone level if the serum hormone concentration of SHBG is reduced to a level that significantly increases the free hormone.
CLINICAL FINDINGS IN HYPERANDROGENISM
Hyperandrogenism is characterized by an abnormally elevated serum concentration of androgens and/or physical findings consistent with androgen excess. Androgenic hormones in the female can stimulate abnormal terminal hair growth, voice and muscle changes, hair loss, clitoral enlargement, and reduction in breast size. Physical characteristics of hyperandrogenism are as follows.
Androgenic Hair Changes
During gestation, the hair follicles of the developing fetus produce fine, unpigmented hair known as lanugo. The total number of hair follicles is determined late in the second trimester of pregnancy. With time, some of the hair follicles produce thick, darkly pigmented terminal hair in response to androgen exposure. The remaining hair follicles produce vellus hair, which are finer and not as darkly pigmented.
Normal hair growth cycle follows three stages: anagen (growth phase), catagen (involution phase), and telogen phase (rest phase).
Hirsutism
Hirsutism is excessive male pattern hair growth in women. It refers to the growth of terminal hair on the face, chest, back, lower abdomen, and upper thighs caused by the overactivity or overexpression of circulating androgens. The abnormal hair growth is predominantly midline. Androgens stimulate hair growth, increase the diameter of the hair shaft, and deepen the pigmentation of the hair. In contrast, estrogens slow hair growth and decrease hair diameter and pigmentation.
Idiopathic hirsutism is the term used when a hirsute individual has normal levels of circulating androgens and has not been diagnosed with polycystic ovarian syndrome (PCOS) or another disorder.
The Ferriman-Gallwey score is an objective tool that may be used in the clinical setting to grade hair growth in women. This method evaluates nine different androgen-sensitive hair growth sites on a scale from 0 to 4. Ninety-five percent of women will have a score under 8. Scores >8 suggest an excess of androgenmediated hair growth and this should be confirmed with a more extensive hormone evaluation.
Hypertrichosis
Hypertrichosis is the generalized, excessive growth of vellus hair. It may be caused by genetic factors, underlying malignancy, or exposure to drugs such as phenytoin, penicillamine, diazoxide, cyclosporine, and minoxidil. It may also be seen with a number of medical conditions, including anorexia nervosa, hypothyroidism, malnutrition, porphyria, dermatomyositis, and paraneoplastic syndromes. Hypertrichosis should not be mistaken for hirsutism.
Hair Loss
Recession of hair in the frontal and temporal regions of the scalp and the crown of the head (i.e., male pattern baldness) in response to androgens is common with aging. This is the most common pattern of hair loss and affects approximately 30% to 40% of men and women alike. However, hair loss is less evident in women because it is typically more diffuse and rarely complete. The fact that excessive androgen activity stimulates hair growth on some parts of the body while causing hair loss from others remains unexplained.
Young men and women with androgenic alopecia have higher levels of 5-alpha reductase, increased androgen receptors, and lower levels of the enzyme cytochrome P-450 aromatase (which converts androgens such as testosterone and 4-androstenedione to the estrogens estradiol and estrone, respectively).
Virilization
This is an appearance of masculine features due to extreme excess androgenic activity. It refers to a constellation of symptoms, including deepening of the voice, male body habitus, male pattern baldness, clitoromegaly, and reduction of breast size.
Virilization is very rare and may be associated with adrenal tumors and hyperplasia or ovarian tumors, such as theca lutein cysts, luteomas, and Sertoli-Leydig cell tumors.
Skin Changes
Androgens stimulate secretions from pilosebaceous glands, resulting in oily skin. Severe acne is a manifestation of excessive androgenic hormone activity.
Voice Changes
The vocal cords can undergo irreversible thickening, resulting in a lower tone of the voice.
Male Body Habitus
Hypertrophy of major muscle groups, such as arm and leg muscles, occurs in response to androgen exposure and may result in the development of a male body habitus.
Clitoromegaly
Enlargement of the clitoris may occur. This is a dose-dependent event and is irreversible. It is more commonly seen when the excessive androgen exposure occurs in childhood or around the time of puberty.
Acanthosis Nigricans
Acanthosis nigricans is a gray-brown, velvety discoloration of the skin that is associated with hyperinsulinemia and obesity. Acanthosis nigricans is typically seen in the groin, neck, axillary, and vulvar regions. These patients should undergo testing for diabetes mellitus. Acanthosis nigricans can also be a paraneoplastic syndrome and associated with an underlying malignancy, commonly an adenocarcinoma involving the gastrointestinal (GI) tract.
DIAGNOSIS OF HYPERANDROGENISM
History and Physical Examination
Hyperandrogenism may be diagnosed if signs of androgen excess are present (see earlier discussion).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


