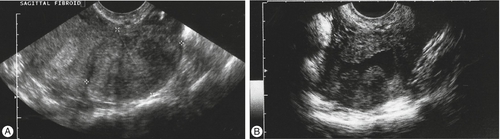
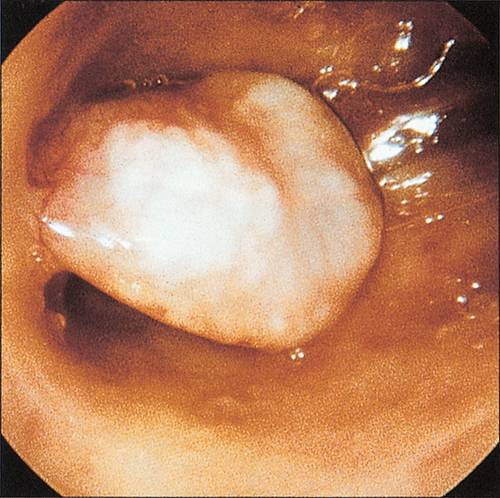
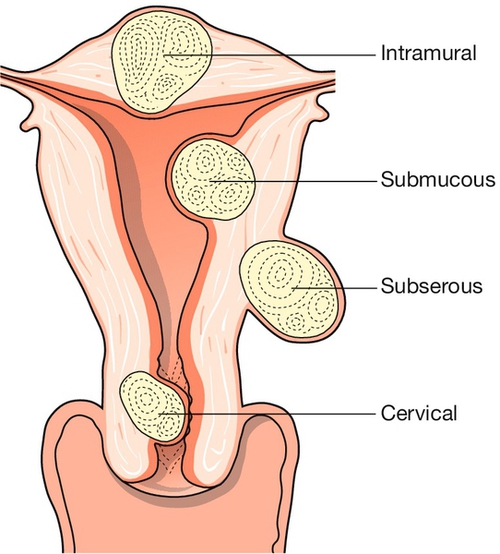
11 Heavy menstrual bleeding (HMB) is defined, for clinical purposes, as bleeding that has an adverse impact on the quality of life of a woman; it may occur alone or with other symptoms. Menstrual blood loss can be measured, but this is usually only performed for research purposes. HMB was often called ‘menorrhagia’ in the past, but this term is better avoided as it means different things to different people, e.g. in the USA the definition is different from that in the UK. HMB is the commonest cause of iron-deficiency anaemia in women in the affluent world. Menstrual problems are becoming more prevalent, since women experience more periods in their lifetime than did their predecessors 100 years ago (approximately 400 periods vs 40). This is because women have fewer children and breastfeed less (lactational amenorrhoea). Only 50% of women who complain of excessive heavy bleeding, however, actually suffer from loss that falls outside the normal range for a population of women not complaining of any menstrual abnormality (> 80 mL/month). The medical and surgical treatment of HMB is also an appreciable burden to health-service resources. HMB is a common indication for hysterectomy, although the numbers have fallen in the last 10 years with the introduction of alternative, effective treatments. Although a commonly performed operation, hysterectomy is a major surgical procedure and its use needs to be balanced against the potential associated mortality and morbidity. Satisfaction rates with hysterectomy are, however, very high. The causes are summarized in Table 11.1. Table 11.1 The main causes of HMB HMB is associated with both benign pathology (e.g. uterine fibroids, endometrial polyps, adenomyosis, pelvic infection) and, extremely rarely, malignant pathology (e.g. endometrial cancer). Over half of those women with an excessively heavy loss of > 200 mL will have fibroids. With the advent of high quality ultrasound that is easily available in outpatient clinics, pathology is identified in a greater proportion of women. Endometrial polyps are common benign localized overgrowths of the endometrium. They consist of a fibrous tissue core covered by columnar epithelium, and it is believed that they arise as a result of disordered cycles of apoptosis and regrowth of endometrium. Although it is uncertain that they cause HMB, it is likely that intrauterine endometrial polyps do increase the likelihood of irregular bleeding (Fig. 11.1). It is unlikely, however, that small endocervical polyps detected at the time of a routine cervical smear cause the same effect. Malignant change of such a polyp is very rare. Uterine fibroids (leiomyomas) are benign tumours of the myometrium, which are present in approximately 20% of women of reproductive age. They are well-circumscribed whorls of smooth muscle cells with collagen and may be single or multiple (Fig. 11.2). Size varies from microscopic growths to tumours that weigh as much as 40 kg and they are more common in women of Afro-Caribbean origin. Sub-mucous fibroids project into the uterine cavity, intramural fibroids are contained within the wall of the uterus, and subserosal fibroids project from the surface of the uterus; cervical fibroids arise from the cervix. Many are asymptomatic, but when symptoms do occur, they are often related to the site and/or size of the fibroid. Presenting symptoms include menstrual dysfunction, infertility, miscarriage, dyspareunia and pelvic discomfort. The mechanism by which fibroids adversely affect reproduction is unclear, but may be related in part to distortion of the uterine cavity affecting implantation. It is unlikely that fibroids not distorting the cavity have an adverse impact. Fibroids may also present because of pressure effects on surrounding organs, such as frequency of micturition as a result of pressure on the bladder, or even hydronephrosis due to ureteric compression. Growth of fibroids is mediated by sex steroids, particularly oestrogen and they therefore grow during pregnancy and shrink after the menopause. Occasionally during pregnancy, necrosis of the fibroid (‘red degeneration’) leads to acute abdominal pain. The incidence of malignant change (leiomyosarcoma) in fibroids is considered to be extremely low (0.1%). This was known in the past as ‘dysfunctional uterine bleeding’, but again, this term should be avoided. HMB in the absence of recognizable pelvic pathology or systemic disease is a diagnosis of exclusion and is probably the commonest ‘diagnosis’ reached after investigating women with HMB. Some HMB with no pathology may be ‘anovulatory’ or ‘ovulatory’, although clinically, this is not an important distinction, as treatment is the same in both cases. The underlying cause is likely to reside at the level of the endometrium, although the precise nature of the vascular and endocrine abnormality remains elusive. Very rarely, HMB is associated with such medical problems as thyroid disease (both hypo- and hyperthyroidism), hepatic disease and renal disease (although the majority of those with end-stage renal failure are amenorrhoeic). Other symptoms of the disorder are likely to be present. Certain coagulation abnormalities (e.g. von Willebrand disease) and platelet defects (e.g. thrombocytopenia) are associated with an increased incidence of HMB. The number of sanitary towels used, duration of bleeding or passage of clots, seems to have little correlation with the actual volume of blood lost. However, complaints of ‘flooding’ (leakage of heavy blood loss onto clothing) and having to use ‘double sanitary protection’ (pad and tampon) to prevent leakage of blood onto clothes are indicative of HMB and are likely to have a negative impact upon the woman’s quality of life. It is important, therefore, to ask about the degree of inconvenience experienced, such as time lost from work, or becoming housebound during menses, owing to fear of social embarrassment from an episode of flooding in public. A history of irregular bleeding, dyspareunia, pelvic pain or intermenstrual or post-coital bleeding may raise the suspicion of underlying pathology and often require additional investigation. They can be termed ‘red light’ symptoms. The woman should also be questioned about symptoms suggestive of anaemia, such as fatigue and light-headedness. A history suggestive of systemic disease such as a thyroid disorder or a clotting abnormality would signal that further investigation for such causes would be required. The woman should also be questioned about risk factors for endometrial cancer, such as use of unopposed oestrogen, tamoxifen use, polycystic ovary syndrome and family history of endometrial or colon cancer. It is also important to establish if she has a history of thromboembolism, as many medical treatments for HMB are hormonal and thus their use may be relatively or absolutely contraindicated. The woman should be examined for signs of anaemia. An abdominal, bimanual and speculum examination should be considered. An enlarged, ‘bulky’ uterus suggests uterine fibroids, and tenderness suggests endometriosis, pelvic inflammatory disease or adenomyosis. A full blood count should be carried out in all women, to diagnose/exclude anaemia. Thyroid function tests and tests of coagulation should be performed only if there are features suggestive of this in the history. No other endocrine tests are routinely indicated. A pelvic ultrasound scan should be performed if history or examination suggests structural uterine pathology, or if it is not possible to assess the uterus clinically because of obesity. The site and size of abnormalities such as fibroids can be determined, together with assessment of the ovaries (Fig. 11.3). (A) A large intramural fibroid. (B) Two submucous fibroids projecting into the cavity of the uterus, which contains a small amount of fluid (saline infusion ultrasound scan).
Heavy menstrual bleeding and dysmenorrhoea
Heavy menstrual bleeding
Causes of HMB
1. Uterine pathology, e.g. fibroids
Common
2. No apparent cause
Very common
3. Medical disorders, including
clotting defects
Very rare
Uterine pathology
HMB in the absence of pathology
Medical disorders and clotting defects
Assessment of HMB
History
Examination
Investigations
Laboratory tests
Ultrasound
Endometrial assessment
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


