Fig. 12.1
ESHRE/ESGE classification of female genital tract anomalies indicating the classes and sub-classes that are associated with health problems
Cyclic Pelvic Pain
Patients with obstructive anomalies, which mainly include Class U4, U5 and complex ones, that is C1, C3, C4, V2, V3 and V4, are asymptomatic until they reach puberty. Then their main presenting symptom is amenorrhea and cyclical abdominal pain, although in cases of fusion defects of the genital tract (e.g. complete bicorporeal uterus with double cervix and longitudinal obstructing vaginal septum – U3b/C2/V2), menstruation from the unilateral horn of the uterus may still occur. Normal secondary sexual characteristics are present.
The accumulation of repeated menstrual content in the vagina creates a hematocolpos. When the obstruction is low enough, as it happens in case of imperforate hymen, the vagina has the capacity to expand considerably, so giving the impression of a pelvic abdominal mass. On the contrary, when the obstruction is high enough in the vagina, due to its restricted expansion capability, the retrograde menstruation is the main complication, which results in cyclic pelvic pain. It is at this time when children or adolescents with obstructive phenomenon come to diagnosis [3]. Sometimes, unilateral cyclic pain, followed by constant pain may be present. These symptoms are found in cases of obstructed hemivagina (V2), which present later than the other obstructing vaginal anomalies, because menstrual flow occurs from the non-obstructed hemi-uterus [4].
Patients who have any obstruction to menstrual flow, are at increased risk for endometriosis. In these cases, the retention of menstrual blood gives place to retrograde menstruation and the deposition of the blood in the pelvic cavity leads to the development of endometriosis, which may be severe and may result in the formation of endometriomas and destruction of pelvic anatomy (Fig. 12.2) [5]. After the relief of obstruction or removal of the non-communicating horn with functional endometrium endometriosis resolves, although it has been described that such removal does not reduce the risk of persistence or recurrence of the disease [6].
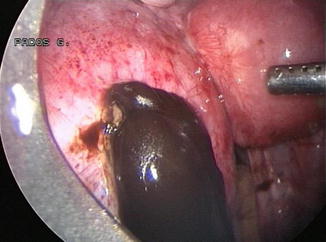
Fig. 12.2
Class U4a hemi uterus, with non-communicating left horn. Endometriosis lesions are noticed in the pouch of douglas (Courtesy of Pados G.)
Ectopic Pregnancy
Unicornuate or Hemi-uterus accounts for approximately 10 % of all Mullerian anomalies and of these Class U4a represents 90 % of all unicornuate uterus [7]. This congenital anomaly is susceptible to many gynecologic and obstetric complications. Pregnancies in the rudimentary horn have been described, they occur when migration of a sperm takes place through the abdominal cavity and show a higher incidence for abortion or rupture of the horn. It has been reported that the incidence of ectopic pregnancy in the non-communicating horn is as high as 22 % [3]. On the contrary, no increase in the frequency of ectopic pregnancies in women with other uterine anomalies has been reported and the incidence in these cases is 1–2 % [8].
A pregnancy conceived in a non-communicating horn has a 70 % chance of rupturing [9]. When rupture of the pregnant rudimentary horn occurs, it is almost always an emergency case. Rupture usually takes place between 10 and 15 weeks of gestation and causes heavy bleeding, thus threatening patient’s life [3]. Although full-term pregnancies in the uterine horn have been reported as early as 1951 [10], its rupture is still a life-threatening complication in pregnancy. Since the incidence of ectopic pregnancies in patients with a non-communicating horn is high and its rupture is a serious complication, laparoscopic removal of the rudimentary horn and its tube is indicated when this uterine anomaly is diagnosed (Fig. 12.3) [7]. Sonographically guided hysteroscopic correction has been, also, proposed in a case report [8], but restoration management should not be considered an alternative approach for the following reasons: (a) there is a considerable variation in the anatomy of the non-communicating horns, so making extrapolation of restoration management not feasible in every case, (b) the muscle of the rudimentary horn is exceptionally thin and therefore placentation frequently pathological (i.e. placenta acreta) and (c) the blood supply of the horn is frequently compromised.
Fig. 12.3
Laparoscopic removal of the left rudimentary horn (Class U4a hemi uterus) with ectopic pregnancy within it (Courtesy of Pados G.)
Renal Abnormalities Occurring with Female Genital Malformations
The association of renal abnormalities with female genital tract malformations has been well recognized and therefore the adequate assessment of the renal tract consists an inevitable part of the routine evaluation of patients presenting with Mullerian anomalies. The incidence of renal anomalies in this group of patients is approximately 30 % [11], with unilateral kidney absence being the most common abnormality, while the incidence of unilateral kidney absence in the normal population is around 1 in 1,000 [12]. However, the incidence of this is not the same across the spectrum of Mullerian anomalies, being the most common in uterus didelphis (U3 C2) [13]. Other less frequent but of clinical significance abnormalities include pelvic ureteric remnants, which insert ectopically, mainly in the vagina, ectopic ureters, which may cause incontinence and infection, scarred kidneys and dysplastic kidney. These abnormalities certainly have clinical implications not only concerning symptomatology, but also for scheduling complex multidisciplinary surgical interventions.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


