Head and Neck Sinuses and Masses
Lesions of the head and neck in children can be subdivided by etiology as those resulting from infection, trauma, neoplasm, or those of congenital origin. The more common benign neoplasms including hemangiomas, lymphangiomas, and cystic hygromas are discussed in Chapter 72. Malignant neoplasms of childhood (e.g., neuroblastoma, lymphoma, and rhabdomyosarcoma), which occur as primary or metastatic masses in the head and neck, lesions of the thyroid and parathyroid, as well as traumatic injuries of the head and neck, also are discussed in other chapters. In this chapter, common congenital head and neck malformations are discussed, and inflammatory lesions are reviewed.
Lesions of Embryonic Origin
Congenital cysts and sinuses in the neck result from embryonic structures that have failed to mature or have persisted in an aberrant fashion.1,2 Both diagnosis and therapy depend on a working knowledge of the embryologic origin and differentiation of the head and neck structures.3,4 This knowledge is particularly important because complete resection of cartilaginous remnants, remnants of the branchial arch and cleft structures, and midline fusion abnormalities is needed to avoid recurrence. Congenital lesions of the head and neck, in descending order of frequency, are thyroglossal duct cysts, preauricular pits and sinuses, branchial cleft anomalies, dermoid cysts, and median cervical clefts.
Thyroglossal Duct Cyst
One of the most common lesions in the midline of the neck is the thyroglossal duct cyst. Thyroglossal duct remnants are found in 7% of the population and most are asymptomatic.4,5 Although embryonic in origin, it is rare for these lesions to manifest in the newborn period.1 More commonly, they are noted in preschool-age children.1 Thyroglossal duct cysts also are common in young adults and, with the exception of thyroid goiter, are the most common midline neck mass.6
The embryogenesis of the thyroglossal duct is intimately involved with that of the thyroid gland, the hyoid bone, and the tongue.7 The foramen cecum is the site of the development of the thyroid diverticulum. In the embryo, this structure develops caudal to the central tuberculum impar, which is one of the pharyngeal buds that leads to the formation of the tongue. As the tongue develops, the thyroid diverticulum descends into the neck, maintaining its connection to the foramen cecum. The hyoid bone is developing from the second branchial arch at this time. The thyroid gland develops between weeks 4 and 7 of gestation and descends into its pretracheal position in the neck.8 As a result of these multiple events occurring simultaneously, the thyroglossal duct may pass in front of or behind the hyoid bone, but most commonly, it passes through it. Normally, the duct disappears by the time the thyroid reaches its appropriate position by 5 to 8 weeks gestation.5,9 Thyroglossal duct cysts never have a primary external opening because the embryologic thyroglossal tract never reaches the surface of the neck.8 A cyst can be located anywhere along the migratory course of the thyroglossal tract if it fails to become obliterated (Fig. 73-1). Occasionally, the cysts attach to the pyramidal lobe or may be intrathyroidal.10 Complete failure of migration of the thyroid results in a lingual thyroid, which develops beneath the foramen cecum at the base of the tongue.11 In this instance, no thyroid tissue is found in the neck.
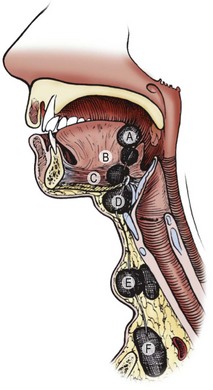
FIGURE 73-1 Thyroglossal duct cysts can be located anywhere from the base of the tongue to behind the sternum. A and B, Lingual (rare); C and D, adjacent to hyoid bone (common); E and F, suprasternal fossa (rare). (From Welch KJ, Randolph JG, Ravitch MM, et al. editors. Pediatric Surgery. 4th ed. Chicago: Year Book Medical; 1986. p. 549.)
Two-thirds of thyroglossal duct anomalies are discovered within the first three decades of life.5 Classically, the thyroglossal cysts are located in the midline at or just below the hyoid bone (Fig. 73-2). Suprahyoid thyroglossal cysts must be distinguished from submental dermoid cysts and from submental lymph nodes.12 Rarely, the cysts are suprasternal in location. The initial sign is usually a painless mass in the midline of the neck, with 66% found adjacent to the hyoid bone.9 On physical examination, the thyroglossal duct cyst is smooth, soft, and nontender. To distinguish this lesion from the more superficial dermoid cyst, one should palpate the lesion while the child sticks out his or her tongue. Owing to its attachment to the foramen cecum, the thyroglossal duct cyst usually moves cephalad when the tongue protrudes. This maneuver is more reliable than asking the child to swallow and determining whether the mass moves with swallowing. Owing to the communication to the mouth via the foramen cecum, thyroglossal cysts can become infected with oral flora. One-third of patients will present with a concurrent or prior infection, and one-quarter will present with a draining sinus from spontaneous or incisional drainage of an abscess.9 Some patients may present with a foul taste in the mouth from spontaneous drainage of the cyst via the foramen cecum.

FIGURE 73-2 A classic thyroglossal duct cyst located in the midline just below the hyoid bone. Markings on the neck represent the thyroid, cricoid and tracheal cartilages.
The preoperative evaluation for a patient with a suspected thyroglossal duct cyst includes a complete history and physical examination. Patients with findings concerning for hypothyroidism should undergo thyroid function testing and additional imaging to exclude median ectopic thyroid. The incidence of ectopic thyroid tissue in or near the duct is reported to be from 10–45%, and some clinicians have advocated preoperative thyroid scanning or ultrasound (US) to eliminate the possibility of an ectopic thyroid gland masquerading as a thyroglossal duct cyst.13–17 Ultrasound appears to be very accurate and avoids the need for radiation and possible sedation in younger children.16 Although ultrasound has been noted to have significant limitations in differentiating thyroglossal duct cysts from other midline neck masses, it can be useful in differentiating cysts and ectopic thyroid.18 Ninety per cent of ectopic thyroid tissue lies at the base of the tongue, and thyroglossal duct cysts are rarely found there. Abnormal thyroid function tests, a suggestive history, or a solid mass on ultrasound should prompt a preoperative thyroid scan to ensure the lesion is not the only thyroid gland present, which occurs in less than 1–2% of thyroglossal duct cysts.9,15,19 If ectopic thyroid tissue is found, the management is controversial, but some clinicians suggest a trial of medical suppression to decrease the size of the mass.19
Elective surgical excision a of thyroglossal duct cyst is advised to avoid the complications of infection and the small risk (<1%) of cancer (papillary thyroid carcinoma) developing in the cyst.15 The operation includes complete excision of the cyst and its tract upward to the base of the tongue (Fig. 73-3), and resection of the central portion of the hyoid bone as described by Sistrunk in 1920.20–22 Several other studies have shown that multiple smaller tracts can connect through the hyoid bone to the floor of the mouth, requiring wide resection of tracts above the hyoid.20–22 If these suprahyoid tracts remain, the incidence of recurrence increases.23 The best chance for successful excision is adequate wide resection at the initial procedure.24

FIGURE 73-3 Complete excision of a previously infected thyroglossal duct cyst. Surrounding skin was removed because of changes related to a previous infection. Note the well-defined tract leading toward the hyoid bone and the floor of the mouth. The operation was completed by excising the central portion of the hyoid bone and suture ligating the tract.
As with all neck surgery, the patient should be supine with the neck slightly hyperextended (Fig. 73-4). The thyroglossal cyst is exposed through a transverse incision. The cyst has a characteristic appearance, distinctly different from that of thyroid tissue. The dissection should continue cephalad to the hyoid, resecting a block of tissue along the tract. Transecting the hyoid is simplified by using angled scissors, similar to Potts scissors, or by using a side-cutting bone cutter. Alternatively, some advocate use of an ultrasonic osteotomy device to minimize trauma to surrounding soft tissues.25 The base of the tract at the floor of the mouth is ligated with absorbable suture. The wings of the hyoid do not need to be approximated. The incision is closed in layers. If the floor of the mouth is entered inadvertently, this can be repaired with absorbable suture. The incision is copiously irrigated. Occasionally, the dissection may be made simpler by having the anesthesiologist place his or her finger at the base of the child’s tongue to identify the cephalad extent of the dissection. With complete excision, including the central portion of the hyoid bone, the risk of recurrence is low, 2–5%.5,9,23,26 Some authors advocate more extensive excision of the infrahyoid tissue as well as exposure of the posterior hyoid space, noting that extensive arborization of thyroglossal ducts exists at all levels, and residual ducts can result in recurrence. Recurrence rates in series employing these extended excisions range from 0–1.67%.27,28 Risk factors for recurrence include simple cyst excision alone (recurrence rates of 38–70%), intraoperative cyst rupture, presence of a cutaneous component secondary to infection, and postoperative wound infections.5,9,29 The cyst is usually connected to the foramen cecum by single or multiple tracts, which pass through the hyoid. Under histologic exam, the duct lining is stratified squamous epithelium or ciliated pseudostratified columnar epithelium, with associated mucus-secreting glands.9 The cyst contains a characteristic glairy mucus.

FIGURE 73-4 Positioning a child for a cervical operation. Hyperextension of the head with support under the shoulders and stabilization with a bean bag keeps the child in a stable position and facilitates exposure. The head of the bed should be elevated 30° to decrease venous pressure in the neck.
Infected cysts or sinuses should be initially managed by treating the infection. The usual route of infection is via the mouth; thus the common organisms are Haemophilus influenzae, Staphylococus aureus, and Staphylococcus epidermidis.9 Directed antibiotic therapy should be initiated. Needle aspiration may be required to decompress the cyst and allow for identification of the organism, but formal incision and drainage should be avoided. This may seed ductal cells outside of the cyst and increase recurrence rates.9 If incision and drainage is required, the incision should be placed so that it can be completely excised during a formal Sistrunk procedure once the infection clears. Excision of acutely infected cysts should be avoided, as recurrence can occur in 25% of patients.30 Three months should be allowed for inflammation to resolve prior to definitive operative treatment.
If a solid mass is found, it should be sent for frozen section to rule out median ectopic thyroid. If it is normal thyroid tissue and there is additional functional thyroid tissue in the normal location, a Sistrunk procedure with excision of the mass should be performed.9 If there is no other thyroid tissue present, management is controversial. One option is to leave the tissue in situ or reposition it into the strap muscles. This is done to prevent the patient from becoming permanently hypothyroid; however, most patients still require thyroid hormone therapy for hypothyroidism or to control the size of the ectopic thyroid. Due to this likely need for long-term therapy and possible malignant degeneration, some surgeons recommend completely excising the ectopic thyroid tissue regardless of the presence or absence of additional thyroid tissue.9 If the mass is found to represent carcinoma, then management is dependent on the extent of disease. The vast majority of cases are papillary carcinoma. If confined to the cyst specimen, it can be adequately treated with a Sistrunk procedure alone.31 More extensive cancers should undergo risk stratification and generally warrant total thyroidectomy and consideration of adjuvant therapy, including radioactive iodine in some cases.32
Remnants of Embryonic Branchial Apparatus
Branchial anomalies represent approximately 30% of congenital neck masses and can present as cysts, sinuses, or fistulae.5,33 They are equally common in males and females and present in childhood or early adulthood.
During weeks 4 to 8 after fertilization, four pairs of well-developed ridges (branchial arches) dominate the lateral cervicofacial area of the human embryo.34 These four pairs are accompanied by two rudimentary pairs, which are analogous to the gill apparatus of fish.2,34 No true gill mechanisms are found in any stage of the human embryo. These pharyngeal arches and clefts are formed without a true connection between the outer ectodermal clefts and the inner endodermal pharyngeal pouches (Fig. 73-5). The mature structures of the head and neck are derivatives of several branchial arches and their intervening clefts.34,35 The clefts and pouches are gradually obliterated by mesenchyme to form those structures. Branchial cleft anomalies result if that process is incomplete.33
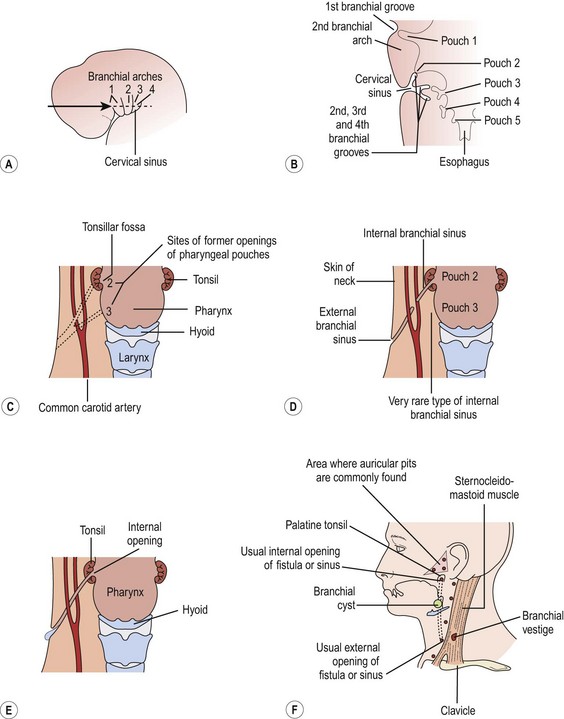
FIGURE 73-5 (A) The head and neck region of a 5-week-old embryo. (B) Horizontal section through the embryo illustrating the relationship of the cervical sinus to the branchial arches and pharyngeal pouches. (C) The child’s neck region, indicating the former sites of openings of the cervical sinus and the pharyngeal pouches. The dotted lines indicate possible courses of branchial fistulas. (D) The embryologic basis of various types of branchial sinuses. (E) A branchial fistula resulting from persistence of parts of the second branchial cleft and the second pharyngeal pouch. (F) Possible sites of branchial cysts and openings of branchial sinuses and fistulas. A branchial vestige also is illustrated. (From Moore KL. The Developing Human: Clinically Oriented Embryology. Philadelphia: WB Saunders; 1977.)
Each arch transforms during gestation into a defined anatomic pattern. Understanding this pattern and its relationship to normal neck structures is key in the diagnosis and treatment of these anomalies. Each anomaly is classified by the cleft or pouch of origin which can be determined by the internal opening of the sinus as well as its relationship to nerves, arteries, and muscles. Careful attention to these relationships is necessary to prevent injury to surrounding tissues and ensure complete resection.33 The embryology and anatomy for each cleft will be discussed later.
Branchial anomalies are lined with either respiratory or squamous epithelium; sinuses and fistulas usually the former and cysts the later.33 One can also see lymphoid tissue, sebaceous glands, salivary tissue or cholesterol crystals. Squamous cell cancer can be seen in adults, but it is rare and it can be difficult to distinguish a primary branchogenic anomaly from a metastatic lesion or an occult primary.5
Complete fistulas are more common than external sinuses. Both are more common than branchial cysts, at least during childhood.36,37 In adults, cysts predominate.36 By definition, all branchial remnants are truly congenital and are present at birth.37,38 Cysts are remnants of sinuses without an external opening and usually appear later in childhood than do sinuses, fistulas, and cartilaginous remnants, which appear in infancy.5,38 Sinuses have the persistence of the external opening only, while fistulas involve the persistence of the branchial groove with breakdown of the branchial membrane.5 Commonly, the tiny external opening of the fistula and the external sinuses remain unnoticed for some time. Spontaneous mucoid drainage from the ostium along the border of the sternocleidomastoid muscle (SCM) usually heralds its presence and initiates the parent’s concern and the reason for the child’s referral. The first clinical presentation may be an infected mass as a result of the inability of the thick mucoid material to drain spontaneously. Infection is, however, less common in fistulas and external sinuses than in cysts.1 The cutaneous openings are occasionally marked by skin tags or cartilaginous remnants. The tract itself may be palpable. A cordlike structure can sometimes be felt ascending in the neck by hyperextending the child’s neck and making the skin taut. Compression along the tract may produce mucoid material exiting from the ostium.
The evaluation of these lesions starts with a thorough history and physical examination. Palpating the tract and observing the mucoid discharge can be confirmatory. Although colored dye or radiopaque material may be injected to delineate the tract, these manipulations generally are unnecessary. Upper endoscopy may be helpful to locate the pharyngeal opening. Both the pyriform sinus and tonsillar fossas should be examined. Cysts may be more difficult to diagnose. They lie deep to the skin along the anterior border of the SCM.1 They can usually be distinguished from cystic hygromas, which are subcutaneous and can be transilluminated. Ultrasound, computed tomography (CT), and magnetic resonance imaging (MRI) can help define the lesion and may be helpful in narrowing the differential diagnosis, but CT is most often used and can demonstrate a fistula in two-thirds of cases.39 Barium esophagram has 50–80% sensitivity for third and fourth branchial fistulas.40 While fine needle aspiration is necessary in adults to exclude metastatic carcinoma, it is not necessary in children and incisional biopsy should be avoided.33
The goal of treating all congenital neck sinuses, cysts, and fistulas is usually complete excision, when no inflammation is present.41 Timing of resection is controversial with some advocating for early resection to prevent infection while others wait until age 2 or 3 years.33,42,43 As with thyroglossal duct cysts, if the lesion is infected at clinical presentation, antibiotic therapy and warm soaks to encourage spontaneous drainage of mucoid plugs should precede definitive excision. Approximately 20% of lesions will have been infected at least once prior to surgery.42 Attempts at complete excision in an inflamed, infected field increase the risk of nerve injury and incomplete resection. Aspiration or limited incision and drainage (I&D) is sometimes necessary to resolve the infection. Complete surgical excision is delayed until the inflammation subsides and the surrounding skin is supple. Endoscopic cauterization of fourth branchial cleft sinuses has been described either at the time of initial abscess drainage or four to six weeks later. Recurrence with this technique seems unusual.44
Surgical resection is performed under general anesthesia with the positioning as shown in Figure 73-4. A small transverse elliptical incision is made around the external opening and deepened beneath the cervical fascia. The initial dissection is along the inferior border of the incision, so that the ascending tract is identified from below and not injured. Placement of a 2-0 or 3-0 monofilament suture or probe within the tract can facilitate dissection. Dissection proceeds cephalad, staying on the tract until visualization of the most superior portion of the tract becomes difficult. At this level, a second, more cephalad, parallel ‘stair-step’ incision or extension of the first incision may be necessary for adequate exposure. The tract is pulled through the second incision, and the dissection is continued cephalad between the bifurcation of the carotid artery to the point where the tract dives into the pharynx. The fistula is suture ligated with absorbable suture. The incision is closed in layers with absorbable sutures. No drains are needed if excision is complete. Recurrences are rare and imply that a portion of the epithelium-lined tract was overlooked. The incidence of recurrence is higher in patients with previously infected lesions. The specific embryology, anatomy, and treatment for each type will now be discussed.
First Cleft Anomalies
The first branchial arch forms the mandible and contributes to the maxillary process of the upper jaw.35,38,45 Abnormal development of the first branchial arch results in a host of facial deformities, including cleft lip and palate, abnormal shape or contour of the external ear, and malformed internal ossicles.35,38 The first branchial cleft contributes to the tympanic cavity, eustachian tube, middle ear cavity, and mastoid air cells. Microtia and aural atresia occur with failure of the first branchial cleft to develop.34,35
First branchial anomalies are rare and account for less than 1% of branchial cleft malformations.33 Cysts are seen as swellings posterior or anterior to the ear or inferior to the earlobe in the submandibular region. External openings, if found, are located inferior to the mandible in a suprahyoid position. One-third open into the external auditory canal.6 The tract may be intimately associated with, or course through, the parotid gland. This association and the proximity of cranial nerve VII make resection difficult, particularly in the younger patient who is likely to have a tract deep to the facial nerve.39 First cleft anomalies are classified as type I or type II (Figs 73-6 and 73-7).5,33 Type I remnants contain only ectoderm, course lateral to the facial nerve, and present as swellings near the ear. Type II lesions consist of both mesoderm and ectoderm, can contain cartilage, pass medial to the facial nerve, and present as swellings inferior to the angle of the mandible or anterior to the SCM in a preauricular, infra-auricular, or postauricular position. First branchial anomalies are more common in females than males and are often misdiagnosed leading to delay in excision.46 Presentation can include cervical, parotid, or auricular signs. Cervical signs include drainage from a pit-like depression at the angle of the mandible. Parotid signs result from rapid enlargement due to inflammation. Auricular signs can consist of swelling or otorrhea.
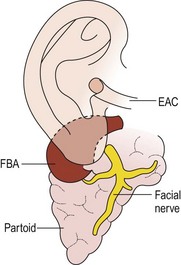
FIGURE 73-6 Type I first branchial cleft anomaly (FBA). Note that the anomaly, located in the parotid gland, has no connection to the external auditory canal (EAC). (From Mukherji SK, Fatterpekar G, Castillo M, et al. Imaging of congenital anomalies of the branchial apparatus. Neuroimaging Clin North Am 2000;10:75–93.)
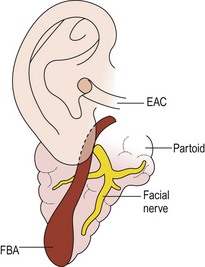
FIGURE 73-7 Type II first branchial cleft anomaly (FBA). The anomaly connects with the external auditory canal (EAC) and extends deep into the parotid gland. (From Mukherji SK, Fatterpekar G, Castillo M, et al. Imaging of congenital anomalies of the branchial apparatus. Neuroimaging Clin North Am 2000;10:75–93.)
Resection of first arch anomalies often requires at least partial facial nerve dissection and superficial parotidectomy. It is important to resect any involved skin or cartilage of the external auditory canal. If it extends medial to the tympanic membrane, a second procedure may be necessary to remove the medial component. Tracts that go to the middle ear are more likely to travel deep or split around the facial nerve.46 A superficial parotidectomy incision allows good exposure and facial nerve monitoring may decrease the risk of nerve injury.47 Another option is to open the fistula tract longitudinally and facilitate the dissection by visualizing it from the inside, but this approach requires microsurgical techniques.48 In any case, identification of the nerve is essential, as the risk of temporary and permanent facial paralysis is significantly higher when the nerve is not identified.49
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


