Germ Cell Tumors
Thomas A. Olson
Germ cell tumors are infrequent tumors in childhood and adolescence. These neoplasms comprise 2% to 3% of all tumors diagnosed in children and adolescents ages 0 to 15 years,1 with an annual incidence of approximately 3 per million. Extracranial germ cell tumors are more common in adolescents 15 to 19 years of age, accounting for 16% of cancer diagnoses in this age group (Fig. 459-1). Ninety percent of germ cell tumors diagnosed during adult life are gonadal, whereas two thirds of childhood germ cell tumors are extragonadal. The age distribution for childhood germ cell tumors is bimodal, with a peak at 3 years of age and a second peak during adolescence. One third of germ cell tumors of childhood are malignant, but most neonatal germ cell tumors, irrespective of location, are benign. However, despite the relative infrequency of malignant tissue, there is a high associated morbidity due to obstruction of airway, hydrops fetalis, and premature delivery.2,3 With advancing age, the proportion of malignant germ cell tumors increases.
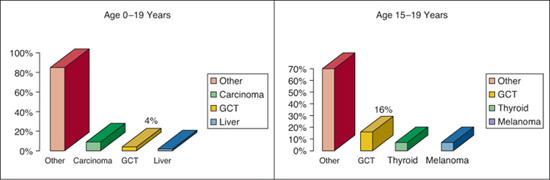
FIGURE 459-1. Germ cell tumors (GCT) in children and adolescents.
ORIGIN OF GERM CELL TUMORS
Germ cell tumors are thought to develop from a common primordial or embryonic germ cell.4 However, there is great heterogeneity in location, histopathology, and genetics.5,6 Tumor development is not well understood but may be related to the stage of germ cell development, the location of stem cells at time of tumorigenesis, and the sex of the individual. During normal development, primordial germ cells migrate from the yolk sac through the mesentery to the gonadal ridge.7 The c-kit receptor and its ligand, stem cell factor-8, have been shown to affect primitive germ cell directional migration to the gonadal ridge. Extragonadal germ cell tumors may develop from primordial germ cells that display an abnormal migration pattern.
Germ cells may give rise to tumors at any point in their migration path or at any stage of differentiation. The pluripotential cells can differentiate into various embryonic or extra-embryonic tissues, which can be either benign or malignant. A mixture of benign and malignant components is common in germ cell tumors, lending support to the notion that different classes of germ cell tumors have a common progenitor. Although there is little doubt that gonadal germ cell tumors are derived from pluripotent descendants of activated germ cells, the origin of extragonadal germ cell tumors is controversial. Cytogenetic studies suggest that such extragonadal tumors may arise from either misplaced pluripotent embryonic tissue or activated germ cells.
CLASSIFICATION
A classification of pediatric germ cell tumors is shown in Table 459-1. Germ cell tumors can be classified into mature or immature teratomas and malignant germ cell tumors.
 MATURE TERATOMA AND IMMATURE TERATOMA
MATURE TERATOMA AND IMMATURE TERATOMA
Mature teratomas are the most common histological subtype of childhood germ cell tumors.8,9 They most often occur in the ovary or extragonadal sites. They usually contain differentiated ectodermal, mesodermal, and endodermal tissue.
Immature teratomas often occur in the ovary near puberty and at extragonadal sites. All three 3 cell layers are often found, but immature tissue (usually neuroepithelial) is present. These are graded 0 to 3 according to immature elements.10
 MALIGNANT GERM CELL TUMOR
MALIGNANT GERM CELL TUMOR
Germinoma
Germinomas are also called seminomas (testicle) or dysgerminomas (ovary). The histology is identical. Germinomas stain strongly for placental alkaline phosphatase. If syncytiotrophoblasts are present, these cells will stain positively for human chorionic gonadotropin beta-subunit (β-HCG). Pure germinomas are the most common malignant germ cell tumor occurring in the central nervous system and ovary.11 Ovarian germinomas are rarely encountered in prepubertal girls.
Yolk Sac Tumor
This is the most common malignant form of childhood germ cell tumor and the only malignant germ cell tumor that occurs in the sacrococcygeal area in infants.12,13 Four histologic patterns have been described, and they often contain Schiller-Duval bodies. Most yolk sac tumors stain positive for alpha-fetoprotein (AFP).
Embryonal Carcinoma
The tumor cells appear epithelial and form large nests. The cells are AFP negative but CD30 positive by immunostaining. Embryonal carcinoma is often found with other malignant elements as part of a mixed germ cell tumor. It is common in adolescent testicular tumors and rarely occurs in children younger than 15 years.
Table 459-1. Germ Cell Tumor Histology
Benign |
Mature teratoma Immature teratoma |
Malignant |
Germinoma
Yolk sac tumor Embryonal carcinoma Choriocarcinoma Gonadoblastoma Mixed germ cell tumor—mature and immature teratoma with malignant elements |



