Fig. 20.1
Organoaxial (a) and mesentericoaxial (b) gastric volvolus. Note the axis of rotation marked by the blue line
Organoaxial:
The stomach rotates around an axis that connects the gastroesophageal junction and the pylorus.
The antrum rotates in opposite direction to the fundus of the stomach.
This is the most common type of gastric volvolus (Fig. 20.2).
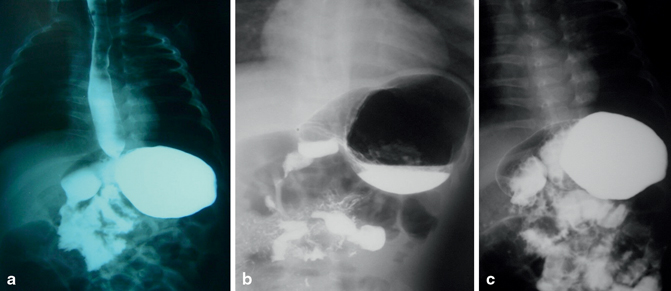
Fig. 20.2
Barium meal showing organo-axial gastric volvolus. Note the associated gastroesophageal reflux in (a) and the air fluid level in (b). Note the absence of gastroesophageal reflux in (c)
Mesentericoaxial:
The stomach rotates around an axis that connects the lesser and greater curvatures. The antrum rotates anteriorly and superiorly so that the posterior surface of the stomach lies anteriorly (Fig. 20.3).
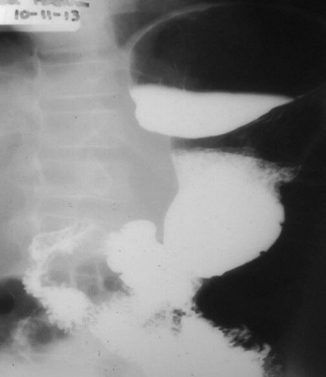
Fig. 20.3
Barium meal showing mesentericoaxial gastric volvolus
Mixed (Combined) :
This is a rare form in which the stomach twists mesentericoaxially and organoaxially.
Combined gastric volvolus is usually observed in patients with chronic volvolus.
The mixed variety is extremely rare and difficult to differentiate both radiologically and intraoperatively.
According to etiology, gastric volvolus is divided into two types:
Type 1 (Idiopathic) :
This type comprises two thirds of cases and is presumably due to abnormal laxity of the gastrosplenic, gastroduodenal, gastrophrenic, and gastrohepatic ligaments. These ligaments anchor the stomach and their laxity leads to volvolus of the stomach.
Type 2 (Secondary or acquired) :
This type is found in one third of patients and is usually associated with congenital or acquired abnormalities that result in abnormal mobility of the stomach. These include:
Diaphragmatic defects
Congenital asplenia
Pyloric stenosis
Colonic distension
Abnormal attachments, adhesions, or bands
Congenital paraesophageal hernia
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


