Fungal Respiratory Infections
Hana Hakim and Aditya H. Gaur
Fungi are ubiquitous in our environment and uncommon respiratory pathogens in the immunocompetent host; they usually present with no or mild symptoms that are self-limiting. In an immunocompromised host these infections can be associated with significant morbidity and mortality. They are categorized into two groups—those that cause endemic mycoses and those classified as opportunistic pathogens (Table 242-1).
EPIDEMIOLOGY
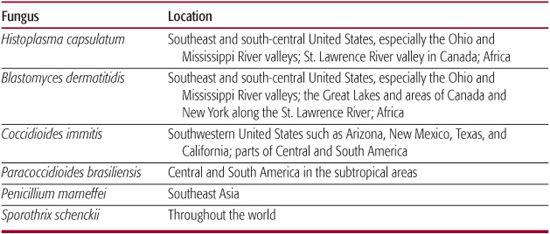
Endemic mycoses are geographically clustered1 as shown in Table 242-2. In cases of suspected infection, past history, including travel, is important because the organisms can remain dormant for many years. Respiratory infections caused by opportunistic fungi generally do not occupy a geographical or ecological niche but are clustered in centers that care for the immunocom-promised host. There seems to be an increase in the incidence of these infections, likely related to an increase in number of immunocompromised patients given intensive antineoplastic and immunosuppressive therapy, related improved survival, increased clinical awareness for these infections, and improved diagnostic ability. The incidence of these infections varies among centers because of factors such as differences in immunosuppressive regimens, transplants, and use of antifungal prophylaxis. 
PATHOGENESIS
Infection is the result of the interplay between host susceptibility, virulence of the pathogen, and inoculum of exposure. Clinical manifestations of infection are in part related to the pathogen and in part the immune system reacting to it. In some sense the organisms causing endemic mycosis are more virulent than those classified as opportunistic pathogens, given their ability to cause disease in the otherwise immunocompetent host.
Deficits in the host defense system that make patients susceptible to fungal respiratory infections can be categorized as (1) neutropenia (as in hematological malignancy, chemotherapy), (2) deficits in cell-mediated immunity (as in AIDS, lymphoma, corticosteroids), (3) deficits in the phagocytic system (as in chronic granulomatous disease), and (4) disruption of the mucosal and cutaneous barriers (as with radiation, chemo-therapy, indwelling catheters). The latter allows resident or colonizing fungal flora (specifically Candida species) access into the bloodstream with dissemination and end organ disease (including the lungs). Inhalation of airborne fungal conidia is the main route of acquiring most other fungal respiratory infections. The alveolar macrophages, activated by different interleukins secreted by T lymphocytes, play a major role in cell-mediated immunity against fungal pathogens. Conidia that are not contained by phagocytes and start mycelial growth trigger a neutrophil response. If these defense systems are impaired, the conidia germinate into the hyphal form in the sinuses or lung tissue (molds) or into yeastlike cells or spherules (dimorphic endemic mycoses).
Table 242–1. Classification of Fungal Pathogens
Opportunistic Fungi |
Opportunistic yeasts |
|
|
|
Filamentous hyaline septate fungi |
|
|
|
Dematiaceous septate fungi (dark molds) |
|
|
|
|
Zygomycetes (aseptate hyphae) |
|
|
|
|
|
|
Endemic Dimorphic Fungi |
|
|
|
|
|
|
aClassified as a fungus rather than a protozoan based on gene sequencing data.
Overall, although qualitative and quantitative defects in the phagocytic system, especially neutrophil and macrophages, seem to make patients especially vulnerable to opportunistic fungi and defects in cell-mediated immunity to endemic mycosis, this predisposition is not absolute. For example, CD4-depleted HIV-infected patients are at high risk for developing Pneumocystis jirovecii pneumonia (PCP). This T-cell depletion also predisposes them to disseminated histoplasmosis, which is an AIDS-defining condition.
Table 242–2. Geographic Locations of the Endemic Mycoses
DIAGNOSIS
The initial clinical findings are nonspecific. Critical to an early diagnosis is a clinician’s index of suspicion, which is influenced by recognition of the host’s immune status and vulnerability for fungal infections. Patient location and travel history aids suspicion of endemic mycosis.
Persistent fever in an immunocompromised host while on broad-spectrum antibiotics, with or without skin lesions and clinically apparent pneumonia or sinusitis, is a common presentation of invasive fungal infection as discussed in Chapter 229.
Although classic clinical findings of inflammation may sometimes be less pronounced in a profoundly neutropenic host, presence of pain (face or chest pain) in a patient with persistent fever on broad-spectrum antibiotics should raise concern about an underlying fungal infection.
The more immunocompromised the host is, the higher the urgency of establishing an accurate diagnosis to identify the infectious organism and initiate appropriate therapy. Disseminated fungal infections that can be detected in blood cultures include Candida species, Histoplasma species, Fusarium species, Trichosporon species, and P. marneffei. A biopsy of a suspicious lesion such as a lung nodule, a pneumonic patch, or a sinus aspirate is often the quickest way to establish a diagnosis and confirm the organism.
A thorough skin exam can be very helpful for the diagnosis of deep-seated invasive fungal infections. Skin lesions are often seen in disseminated candidiasis, aspergillosis, and fusariosis and when present are readily accessible to skin biopsy.
 CLINICAL DIAGNOSIS
CLINICAL DIAGNOSIS
Sinusitis
None of the endemic mycosis are typically present with sinusitis. Invasive fungal sinusitis in immune-compromised patients is most frequently associated with mold infections. Aspergillus species are the most common fungal pathogen involving the nose and paranasal sinuses. Other emerging fungal pathogens such as Fusarium species, Scedosporium species, and zygomycosis have been increasingly reported. Indolent sinus aspergilloma is a localized disease without bone erosion and without predisposing factors of immunodeficiency. Patients present with symptoms of chronic nasal congestion and obstruction or chronic rhinorrhea. On the other hand, aspergillus sinusitis can be an invasive disease with bone erosion. It usually affects immunocompromised patients, being more common in stem cell than solid organ transplant recipients, and most commonly caused by A fumigatus and A flavus. Symptoms and signs include fever, facial pain and tenderness, epistaxis, headache, nasal congestion. and periorbital swelling. Clinical exam of the nares for fungal lesions and a nares fungal culture can help in the diagnosis. Infection is often complicated by hyphal invasion into contiguous structures such as the blood vessels, brain, and orbits, leading to mental status changes, focal neurologic signs, infarction, hemorrhage, or proptosis.
Pulmonary Nodules and Cavities
 A pulmonary nodule detected as a chance radiological finding in an otherwise asymptomatic host may be a presentation of some of the endemic mycosis such as histoplasmosis, a setting in which no treatment is necessary. In contrast, aggressive mold infections in immunocompromised hosts start as a small localized nodule detected only on a chest CT and rapidly progress to more classic findings of pneumonia and related morbidity and mortality if left untreated. In contrast again is an aspergilloma, a solid rounded mass within a pulmonary cavity containing intertwined aspergillus hyphae matted together with fibrin, mucus, and cellular debris. (See Chapter 295.)
A pulmonary nodule detected as a chance radiological finding in an otherwise asymptomatic host may be a presentation of some of the endemic mycosis such as histoplasmosis, a setting in which no treatment is necessary. In contrast, aggressive mold infections in immunocompromised hosts start as a small localized nodule detected only on a chest CT and rapidly progress to more classic findings of pneumonia and related morbidity and mortality if left untreated. In contrast again is an aspergilloma, a solid rounded mass within a pulmonary cavity containing intertwined aspergillus hyphae matted together with fibrin, mucus, and cellular debris. (See Chapter 295.)
Pneumonia
Patients with pneumonia due to endemic mycosis may have a wide spectrum of presentations ranging from being asymptomatic to typical symptoms of fever, cough, dyspnea, and pleuritic chest pain or prolonged pneumonia refractory to antibiotics or adult respiratory distress syndrome. To a large extent this depends on host immune status and the inoculum of organisms inhaled.
In the immunocompetent patient, the most common clinical presentation of coccidioidomycosis is primary pulmonary disease, which is self-limited acute or subacute community-acquired pneumonia 1 to 3 weeks after infection. Five to 10% of these infections result in residual pulmonary lesions such as nodules or cavities. Other clinical manifestations include chronic progressive pulmonary coccidioidomycosis and pulmonary manifestations of disseminated disease. Acute pulmonary infection by Blastomyces dermatitidis usually presents with mild flulike symptoms that resolve spontaneously. However, most patients diagnosed with blastomycosis present with acute or indolent onset chronic pneumonia that manifests as alveolar infiltrates, mass lesions that mimic malignancy, or fibronodular interstitial infiltrates. Most cases of histoplasmosis are asymptomatic, but clinical presentation can include acute pneumonia, mediastinal granulomatous inflammation and fibrosis, chronic progressive pulmonary cavitary disease, or disseminated disease.
A pulmonary presentation of an endemic mycosis in an immunocompromised host can be related to either a primary infection or reactivation of latent infection. Findings can include acute severe pulmonary infection and adult respiratory distress syndrome with or without dissemination.
All of the opportunistic fungi can present with a pneumonic picture that is clinically apparent or found on chest radiology in an immunocom-promised host with persistent fevers.
Other Pulmonary Presentations
Allergic bronchopulmonary aspergillosis (ABPA) is a hyper-sensitivity reaction in the respiratory tract to A fumigatus hyphae that become trapped in the thick mucus of patients with asthma or cystic fibrosis. The primary diagnostic criteria are: (1) episodic bronchial obstruction (asthma), (2) peripheral blood eosinophilia, (3) immediate scratch test reactivity to Aspergillus antigen, (4) precipitating antibodies to Aspergillus antigen, (5) elevated serum IgE concentrations, (6) history of pulmonary infiltrates, and central bronchiectasis. Presence of 6 diagnostic criteria makes the diagnosis highly likely, whereas the presence of all 7 criteria makes the diagnosis certain.11
 RADIOLOGIC DIAGNOSIS
RADIOLOGIC DIAGNOSIS
Although the chest x-ray has the advantage of being quick, widely available, and inexpensive and having a low radiation dose, it has a low sensitivity in the early detection of pneumonia in immunocompromised hosts.12-14
Chest computed tomography (CT) scan is more useful for early detection of lung nodules suggestive of invasive fungal infection and for defining the location, type, and extent of pulmonary lesions to facilitate tissue sampling.15-18 In one study, a CT scan was shown to have 87% sensitivity and 88% negative predictive value as a screening method to exclude pneumonia.15 CT scan findings in pulmonary fungal infections can be variable, including diffuse interstitial infiltrates, discrete nodules, halo sign, air-crescent sign, cavitary lesion, and lobar pneumonia (Fig. 242-1).17,19,20 The halo sign is an area of low attenuation surrounding a nodule caused by edema or bleeding surrounding an ischemic area and has been shown to have high specificity (93%) but low sensitivity of 68% for invasive fungal infection. On follow-up CTs, especially with neutrophil count recovery, the more specific air-crescent sign caused by retraction of infected tissue appears.17 Although the halo sign and the air-crescent sign are seen with invasive pulmonary aspergillosis, these signs are not specific for this fungus and can be seen with other molds.
Differential diagnosis of radiographic changes in the chest of an immunocompromised patient is often broad and, depending on whether it is a lung nodule or pneumonia, includes other nonfungal infectious etiologies such as Nocardia species, tuberculosis, and atypical mycobacteria in addition to noninfectious etiologies including graft-versus-host disease, radiation pneumonitis, drug toxicity, tumor recurrences, and pulmonary hemorrhage.
 LABORATORY DIAGNOSIS
LABORATORY DIAGNOSIS
Microbiologic Testing
Although detectable fungemia occurs with some fungal pathogens such as Candida species, Histoplasma species, Fusarium species, Trichosporon species, and P marneffei, the yield of blood cultures is variable. In an immunosuppressed host, definitive diagnosis is often based on tissue histopathology and/or culture. Obtaining a specimen for these tests requires invasive procedures such as a sinus aspirate, bronchoalveolar lavage (BAL), or lung biopsy. In immunosuppressed patients, the reported diagnostic yield of BAL varies between 30% and 57% but this may improve with the use of fungal polymerase chain reactions and antigen tests such as galactomannan on BAL specimens. A negative BAL result does not exclude fungal infection. Depending on the location of a pulmonary lesion and available expertise, a biopsy can be transbronchial, percutaneous (fine-needle aspiration), or open lung. CT-guided fine-needle aspiration for peripherally located lung nodules is sometimes the preferred first-line approach.23 Although histopathology may show characteristic morphology of an organism, a definitive diagnosis requires growth in cultures and subsequent identification. For example, Aspergillus species, Fusarium species, and Pseudallescheria boydii have similar tissue appearance (septate, branching hyphae) and can be differentiated only by culture.
Serologic Testing
Antigen detection assays are useful for the diagnosis of aspergillosis. These include enzyme immunoassay (EIA) for detection of galactomannan and (1→3)-β-D-glucan, fungal membrane polysaccharides (eTable 242.1  ). These tests have been studied and used as serial assays in a high-risk host and not as a onetime diagnostic test in a patient with a suspected respiratory fungal infection. False-positive results are another limitation of these tests.
). These tests have been studied and used as serial assays in a high-risk host and not as a onetime diagnostic test in a patient with a suspected respiratory fungal infection. False-positive results are another limitation of these tests.
In the case of cryptococcosis, a positive serum cryptococcal antigen test has high sensitivity and specificity for the diagnosis of disseminated disease. Similarly, histoplasma antigen can be detected by enzyme immunoassay in the urine in > 90% of patients and in the serum in > 80% of patients with disseminated histoplasmosis, but it has much less sensitivity in localized diseases such as pulmonary or mediastinal disease.
Antibody detection assays play an important role in the diagnosis of endemic mycoses. However, titers are diagnostic weeks after infection and there may be cross-reacting antibodies that make test result interpretation difficult. A fourfold increase between the acute and convalescent titers is diagnostic. Additionally, the value of antibody detection tests in the diagnosis of endemic mycosis in an immunocompromised patient is limited, given the inability in many cases to mount an antibody response. Molecular diagnostic techniques for fungal pathogens, such as polymerase chain reaction, are still experimental. In one study for invasive pulmonary aspergillosis as compared to galactomannan and β-glucan enzyme immunoassay tests, a fungal polymerase chain reaction (blood) was found to be faster, with better specificity (92%) but variable sensitivity.27

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


