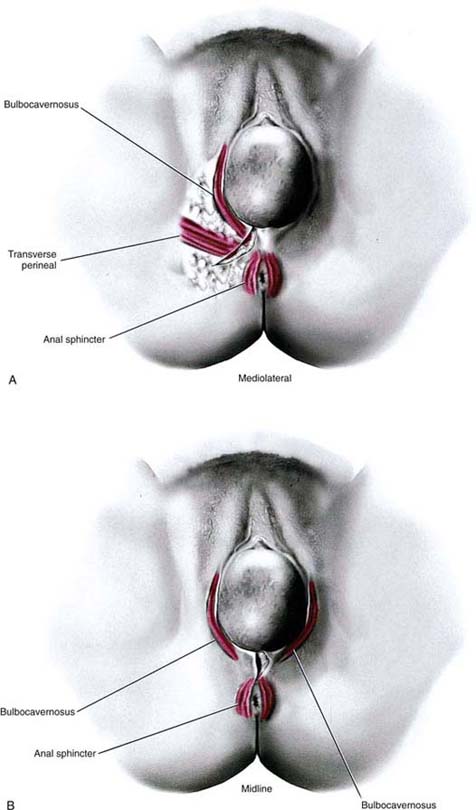
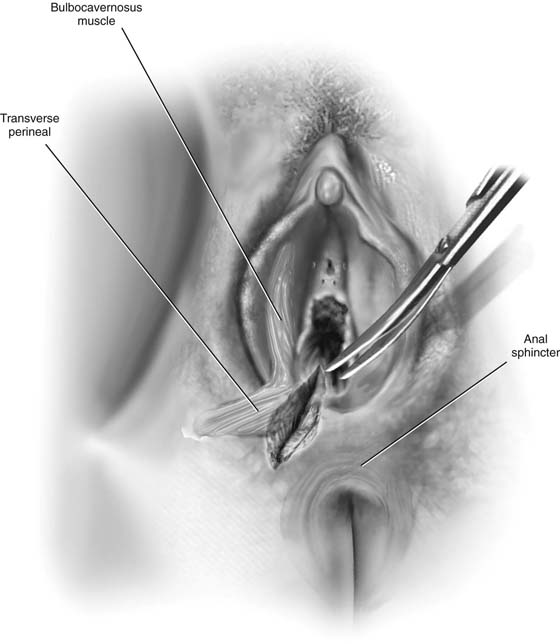
CHAPTER 80 In the United States, episiotomy had been performed routinely when coupled with preterm or full-term obstetric delivery. Recently, the benefits of this operation have been questioned. The risk of third- or fourth-degree lacerations has been shown to be significantly greater, particularly with midline (median) episiotomies versus no episiotomy. No conclusive evidence has yet been published showing that routine (nonselective) episiotomy performance is associated with significantly diminished risks of later pelvic floor dysfunction. A large volume of data verifies that selective episiotomy is beneficial insofar as it avoids anal sphincter injury and diminishes later pelvic floor problems. Most recent reports favor mediolateral over medial (midline) episiotomy because of the decreased risk of third- and fourth-degree tears. Although cutting an episiotomy is an “operation,” its historical performance at best can be described as rugged, and its repair most charitably depicted as casual. For this operation, acceptable precepts appropriate for every surgical procedure should be followed. The latter include knowledge of anatomy, sterile technique, careful tissue handling, sharp and minimally traumatic dissection, control of bleeding, avoidance of tissue devitalization, and anatomic-physiologic reconstruction. The goal of the surgeon under all circumstances should be to cut an episiotomy when required to implement easy, atraumatic delivery while minimizing the risk(s) for third- or fourth-degree lacerations. The bizarre practice of purposely cutting a midline episiotomy and extending it into the rectum should be relegated to the archives of past history. This procedure cuts or creates an incision directed from the right or left lower vagina (at the level of the hymenal ring), through the vestibule, and through the lowest margin of the labium majus, where it joins the perineum, and into the ischiorectal fossa. The operation may include any portion of the structures noted earlier. It is vectored in a direction approximately 45° to 50° from the midline and may include all of the previously mentioned structures (Fig. 80–1). The lower portion of the bulbocavernosus muscle is always cut, and if the incision is extended, the transverse perineal muscle will also be cut (Fig. 80–2). During pregnancy, every one of these structures has an excellent blood supply. Cut vessels in the subcutaneous tissues, fascia, and muscles can bleed briskly and therefore must be clamped and ligated to avoid moderate or even substantial blood loss. The episiotomy cut is usually made with scissors. The operator’s fingers should be inserted between the vagina/vestibule and the baby’s head to protect the latter from injury. The incision, if made correctly and according to previously cited instructions, will clearly avoid injury to the anal sphincter muscle and rectum. It is directed away from those structures. Following delivery of the infant while placental separation is awaited, the incision should be tamponaded with pressure via an abdominal pad(s). Bleeding vessels should be clamped and suture-ligated with 3-0 Vicryl. The cut bulbocavernosus muscle margins should be secured with Allis clamps. Fascial edges at the level of the transverse perineal muscle should be secured with Allis clamps. After the placenta has been delivered, the wound is closed with 2-0 or 3-0 Vicryl sutures approximating the muscles and fascia; 3-0 Vicryl closes Colles’ fascia and subcutaneous tissue, and 3-0 Vicryl is placed through the skin (Figs. 80–3 and 80–4). FIGURE 80–1 The two types of episiotomy, which may be cut at the time of vaginal birth, are illustrated here. Key perineal muscles have been superimposed. A. Mediolateral approach. B. Midline approach. FIGURE 80–2 A right mediolateral episiotomy has been cut. The superimposed bulbocavernosus and transverse perineal muscles have been cut as a result of the direction of the incision. If the episiotomy extends, it will be vectored into the ischiorectal fossa and not into the external sphincter ani.
Episiotomy
Mediolateral Episiotomy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


